

Complement C3-Targeted Therapy: Replacing Long-Held Assertions with Evidence-Based Discovery
- PMID: 28416449
- PMCID: PMC5447467
- DOI: 10.1016/j.it.2017.03.003
Complement C3-Targeted Therapy: Replacing Long-Held Assertions with Evidence-Based Discovery
Abstract
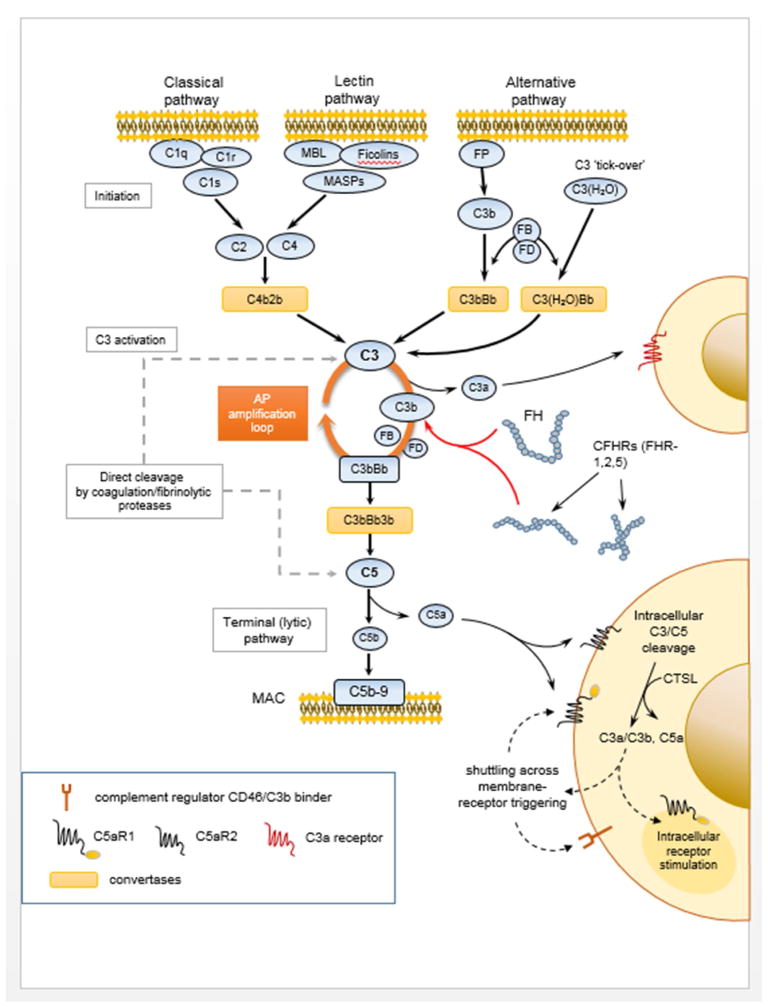
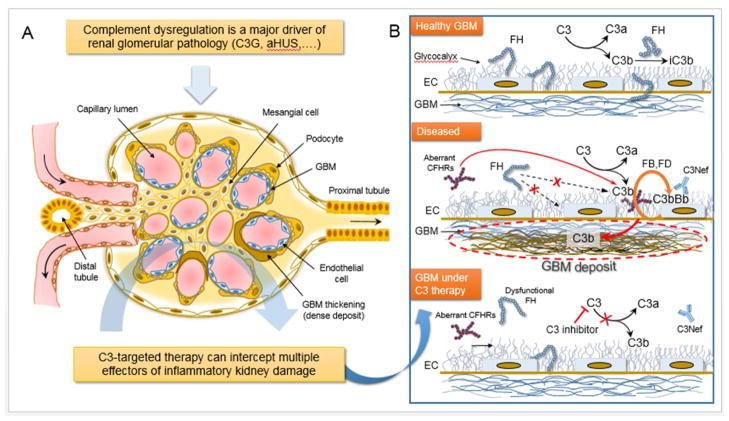
Complement dysregulation underlies several inflammatory disorders, and terminal complement inhibition has thus far afforded significant clinical gains. Nonetheless, emerging pathologies, fueled by complement imbalance and therapy-skewing genetic variance, underscore the need for more comprehensive, disease-tailored interventions. Modulation at the level of C3, a multifaceted orchestrator of the complement cascade, opens up prospects for broader therapeutic efficacy by targeting multiple pathogenic pathways modulated by C3-triggered proinflammatory crosstalk. Notably, C3 intervention is emerging as a viable therapeutic strategy for renal disorders with predominantly complement-driven etiology, such as C3 glomerulopathy (C3G). Using C3G as a paradigm, we argue that concerns about the feasibility of long-term C3 intervention need to be placed into perspective and weighed against actual therapeutic outcomes in prospective clinical trials.
Keywords: AMY-101; C3 glomerulopathy; C3 inhibitors; anti-C5 therapy; clinical efficacy; compstatin.
Published by Elsevier Ltd.
Conflict of interest statement
J.D.L., D.R. and R.J.S. are the inventors of patents and/or patent applications that describe complement inhibitors and/or their use for therapeutic purposes. J.D.L. is the founder of Amyndas Pharmaceuticals, which is developing complement inhibitors for clinical applications. The remaining authors declare no competing financial interests.
Figures
Similar articles
-
Compstatin analog Cp40 inhibits complement dysregulation in vitro in C3 glomerulopathy.Immunobiology. 2015 Aug;220(8):993-8. doi: 10.1016/j.imbio.2015.04.001. Epub 2015 May 5. Immunobiology. 2015. PMID: 25982307 Free PMC article.
-
Complement inhibition in C3 glomerulopathy.Semin Immunol. 2016 Jun;28(3):241-9. doi: 10.1016/j.smim.2016.06.002. Epub 2016 Jul 9. Semin Immunol. 2016. PMID: 27402056 Review.
-
From orphan drugs to adopted therapies: Advancing C3-targeted intervention to the clinical stage.Immunobiology. 2016 Oct;221(10):1046-57. doi: 10.1016/j.imbio.2016.06.013. Epub 2016 Jun 16. Immunobiology. 2016. PMID: 27353192 Free PMC article. Review.
-
Monitoring of complement activation biomarkers and eculizumab in complement-mediated renal disorders.Clin Exp Immunol. 2017 Feb;187(2):304-315. doi: 10.1111/cei.12890. Epub 2016 Nov 25. Clin Exp Immunol. 2017. PMID: 27784126 Free PMC article.
-
Complement therapeutics in inflammatory diseases: promising drug candidates for C3-targeted intervention.Mol Oral Microbiol. 2016 Feb;31(1):3-17. doi: 10.1111/omi.12129. Epub 2015 Oct 7. Mol Oral Microbiol. 2016. PMID: 26332138 Free PMC article. Review.
Cited by
-
A potent complement factor C3-specific nanobody inhibiting multiple functions in the alternative pathway of human and murine complement.J Biol Chem. 2018 Apr 27;293(17):6269-6281. doi: 10.1074/jbc.RA117.001179. Epub 2018 Mar 1. J Biol Chem. 2018. PMID: 29497000 Free PMC article.
-
Small-animal blood exchange is an emerging approach for systemic aging research.Nat Protoc. 2022 Nov;17(11):2469-2493. doi: 10.1038/s41596-022-00731-5. Epub 2022 Aug 19. Nat Protoc. 2022. PMID: 35986217 Free PMC article. Review.
-
Novel Assays to Distinguish Between Properdin-Dependent and Properdin-Independent C3 Nephritic Factors Provide Insight Into Properdin-Inhibiting Therapy.Front Immunol. 2019 Jun 17;10:1350. doi: 10.3389/fimmu.2019.01350. eCollection 2019. Front Immunol. 2019. PMID: 31263464 Free PMC article.
-
The Challenges and Promise of Complement Therapeutics for Ocular Diseases.Front Immunol. 2019 May 15;10:1007. doi: 10.3389/fimmu.2019.01007. eCollection 2019. Front Immunol. 2019. PMID: 31156618 Free PMC article. Review.
-
Clinical promise of next-generation complement therapeutics.Nat Rev Drug Discov. 2019 Sep;18(9):707-729. doi: 10.1038/s41573-019-0031-6. Epub 2019 Jul 19. Nat Rev Drug Discov. 2019. PMID: 31324874 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
