

Long-term cost reduction of routine medications following a residential programme combining physical activity and nutrition in the treatment of type 2 diabetes: a prospective cohort study
- PMID: 28416496
- PMCID: PMC5775459
- DOI: 10.1136/bmjopen-2016-013763
Long-term cost reduction of routine medications following a residential programme combining physical activity and nutrition in the treatment of type 2 diabetes: a prospective cohort study
Abstract
Objectives: To demonstrate that lifestyle modifications will reduce the cost of routine medications in individuals with type 2 diabetes (T2D), through a mechanism involving glycaemic control.
Design: A within-trial cost-medication analysis with a 1-year time horizon.
Setting: Controlled environment within the spa resort of Chatel-Guyon, France.
Participants: Twenty-nine participants (aged 50-70 years) with T2D.
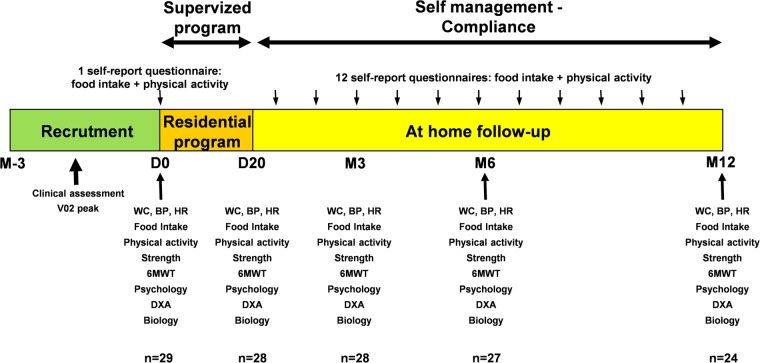
Interventions: A 1-year follow-up intervention, beginning with a 3-week residential programme combining high exercise volume (15-20 hours/week), restrictive diet (-500 kcal/day) and education. Participants continued their routine medication, independently managed by their general practitioner.
Main outcome measures: Number of medications, number of pills, cost of medications and health-related outcomes.
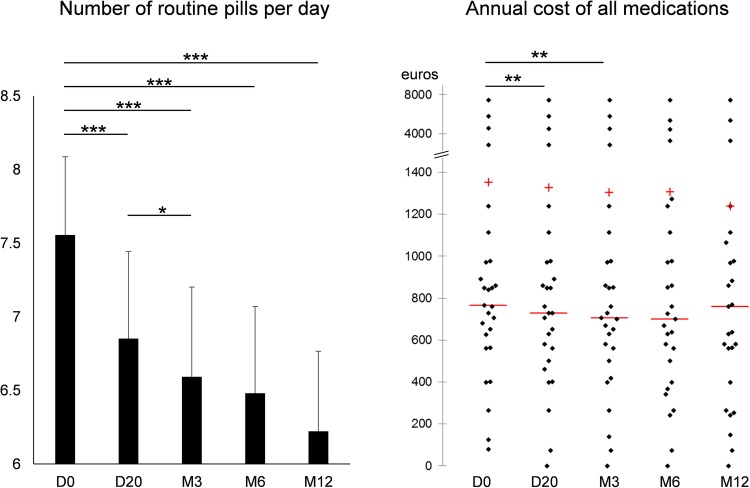
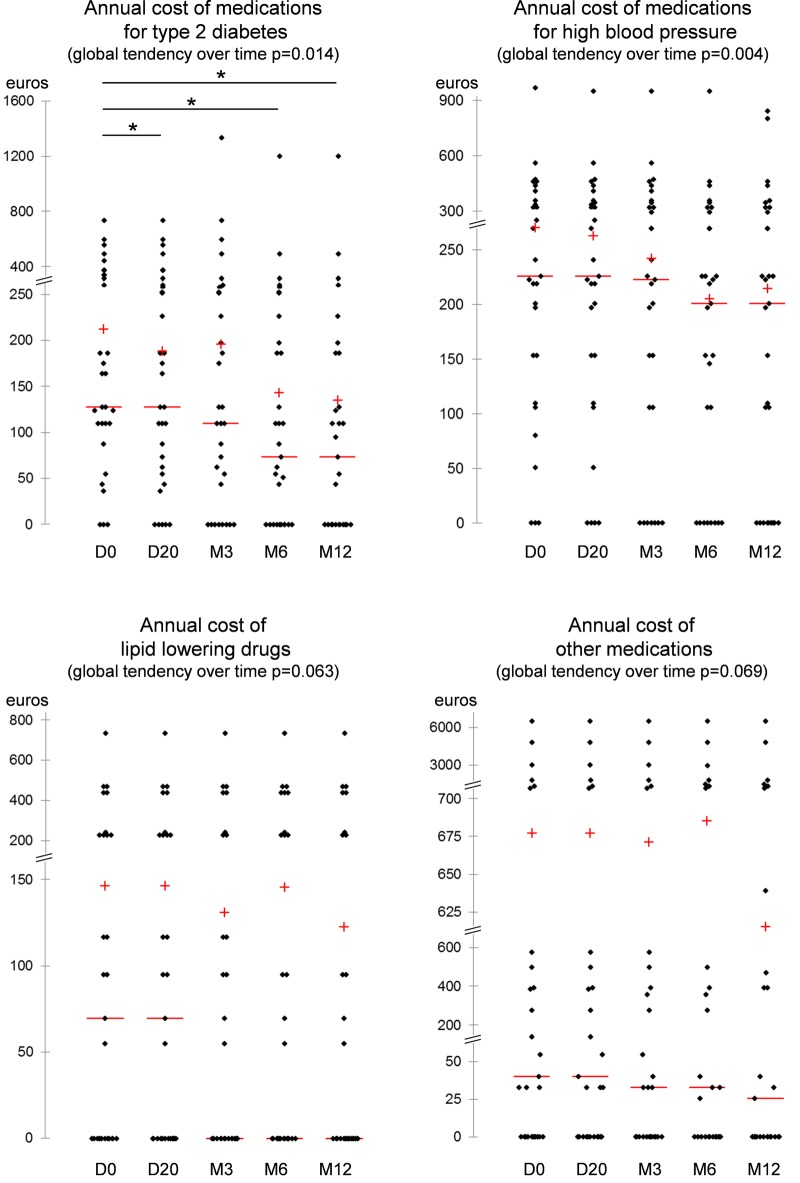
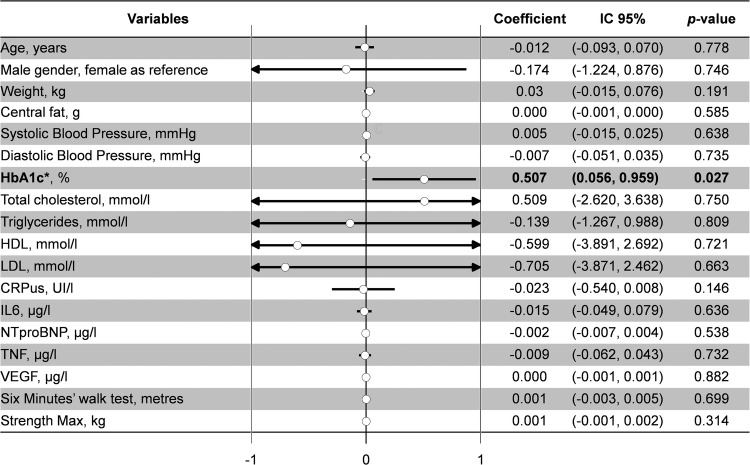
Results: Twenty-six participants completed the 1-year intervention. At 1 year, 14 patients out of 26 (54%) stopped/decreased their medications whereas only 5 (19%) increased or introduced new drugs (χ2=6.3, p=0.02). The number of pills per day decreased by 1.3±0.3 at 12 months (p<0.001). The annual cost of medications for T2D were lower at 1 year (€135.1±43.9) versus baseline (€212.6±35.8) (p=0.03). The regression coefficients on costs of routine medication were 0.507 (95% CI 0.056 to 0.959, p=0.027) for HbA1c and 0.156 (95% CI -0.010 to 0.322, p=0.06) for blood glucose levels. Diabetics patients with HbA1c >6.5% in the highest (last) quartile doubled their routine medication costs (66% vs 33%, p=0.037).
Conclusions: Individuals with T2D reduced routine medication costs following a long-term lifestyle intervention that started with a 3-week residential programme. Combining high exercise volume, restrictive diet and education effectively supported the health of T2D. The main factor explaining reduced medication costs was better glycaemic control, independent of weight changes. Despite limitations precluding generalisability, cost-effective results of reduced medication should contribute to the evidence base required to promote lifestyle interventions for individuals with T2D.
Trial registration number: NCT00917917; Post-results.
Keywords: MEDICAL EDUCATION & TRAINING; NUTRITION & DIETETICS.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Competing interestsNone declared.
Figures
Similar articles
-
Head-to-head comparison of intensive lifestyle intervention (U-TURN) versus conventional multifactorial care in patients with type 2 diabetes: protocol and rationale for an assessor-blinded, parallel group and randomised trial.BMJ Open. 2015 Dec 9;5(12):e009764. doi: 10.1136/bmjopen-2015-009764. BMJ Open. 2015. PMID: 26656025 Free PMC article. Clinical Trial.
-
Cost-Effectiveness of Three Doses of a Behavioral Intervention to Prevent or Delay Type 2 Diabetes in Rural Areas.J Acad Nutr Diet. 2020 Jul;120(7):1163-1171. doi: 10.1016/j.jand.2019.10.025. Epub 2019 Dec 30. J Acad Nutr Diet. 2020. PMID: 31899170 Free PMC article. Clinical Trial.
-
Repaglinide : a pharmacoeconomic review of its use in type 2 diabetes mellitus.Pharmacoeconomics. 2004;22(6):389-411. doi: 10.2165/00019053-200422060-00005. Pharmacoeconomics. 2004. PMID: 15099124 Review.
-
Impact of co-payment level increase of antidiabetic medications on glycaemic control: an interrupted time-series study among Finnish patients with type 2 diabetes.BMC Health Serv Res. 2020 Nov 27;20(1):1095. doi: 10.1186/s12913-020-05952-6. BMC Health Serv Res. 2020. PMID: 33246453 Free PMC article.
-
Behavioural modification interventions for medically unexplained symptoms in primary care: systematic reviews and economic evaluation.Health Technol Assess. 2020 Sep;24(46):1-490. doi: 10.3310/hta24460. Health Technol Assess. 2020. PMID: 32975190 Free PMC article.
Cited by
-
Evaluation of the Clinical and Economic Effects of a Primary Care Anchored, Collaborative, Electronic Health Lifestyle Coaching Program in Denmark: Protocol for a Two-Year Randomized Controlled Trial.JMIR Res Protoc. 2020 Jun 25;9(6):e19172. doi: 10.2196/19172. JMIR Res Protoc. 2020. PMID: 32584260 Free PMC article.
-
Hospitalization and ambulatory costs related to breast cancer due to physical inactivity in the Brazilian state capitals.PLoS One. 2022 Jan 19;17(1):e0261019. doi: 10.1371/journal.pone.0261019. eCollection 2022. PLoS One. 2022. PMID: 35045087 Free PMC article.
-
Dietary Fibres and the Management of Obesity and Metabolic Syndrome: The RESOLVE Study.Nutrients. 2020 Sep 23;12(10):2911. doi: 10.3390/nu12102911. Nutrients. 2020. PMID: 32977595 Free PMC article. Clinical Trial.
-
Italian guidelines for the treatment of type 2 diabetes.Acta Diabetol. 2022 May;59(5):579-622. doi: 10.1007/s00592-022-01857-4. Epub 2022 Mar 15. Acta Diabetol. 2022. PMID: 35288805 Free PMC article. No abstract available.
-
Administration of Jerusalem artichoke reduces the postprandial plasma glucose and glucose-dependent insulinotropic polypeptide (GIP) concentrations in humans.Food Nutr Res. 2022 Apr 4;66. doi: 10.29219/fnr.v66.7870. eCollection 2022. Food Nutr Res. 2022. PMID: 35440936 Free PMC article.
References
-
- Association AD. Diabetes statistics. November 3, 2004.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical