

Restarting Anticoagulant Therapy After Intracranial Hemorrhage: A Systematic Review and Meta-Analysis
- PMID: 28416626
- PMCID: PMC5699447
- DOI: 10.1161/STROKEAHA.116.016327
Restarting Anticoagulant Therapy After Intracranial Hemorrhage: A Systematic Review and Meta-Analysis
Abstract
Background and purpose: The safety and efficacy of restarting anticoagulation therapy after intracranial hemorrhage (ICH) remain unclear. We performed a systematic review and meta-analysis to summarize the associations of anticoagulation resumption with the subsequent risk of ICH recurrence and thromboembolism.
Methods: We searched published medical literature to identify cohort studies involving adults with anticoagulation-associated ICH. Our predictor variable was resumption of anticoagulation. Outcome measures were thromboembolic events (stroke and myocardial infarction) and recurrence of ICH. After assessing study heterogeneity and publication bias, we performed a meta-analysis using random-effects models to assess the strength of association between anticoagulation resumption and our outcomes.
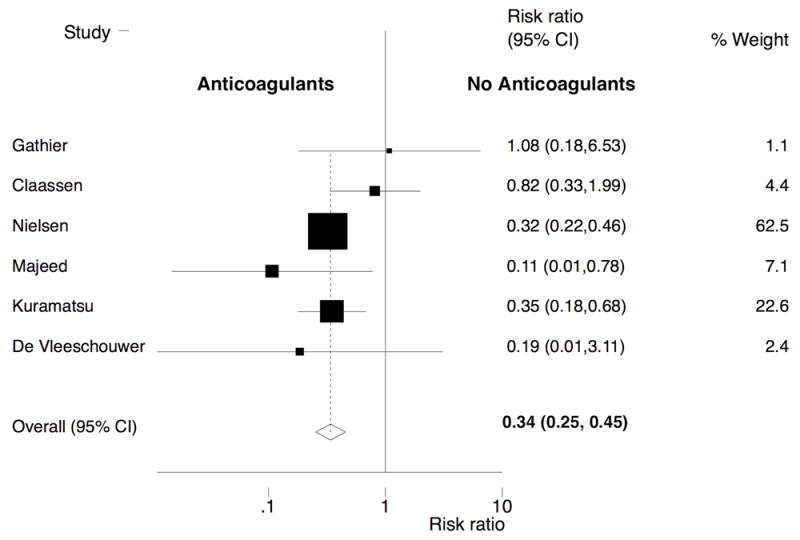
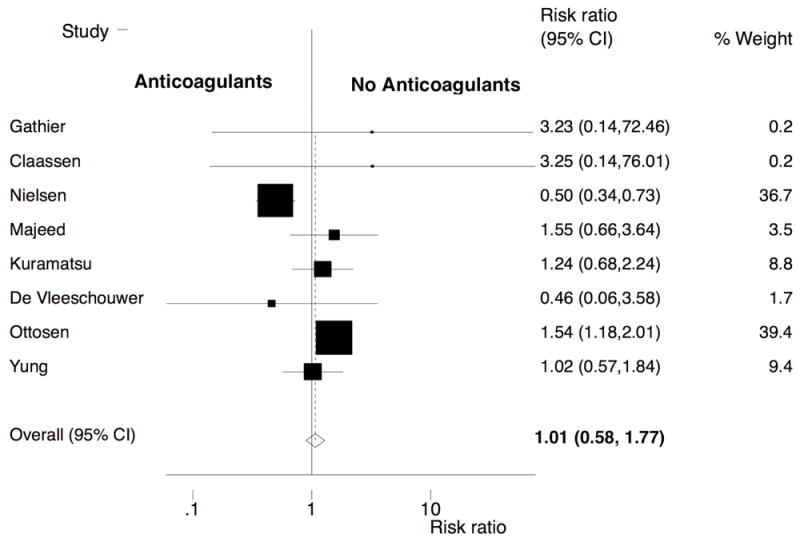
Results: Eight studies were eligible for inclusion in the meta-analysis, with 5306 ICH patients. Almost all studies evaluated anticoagulation with vitamin K antagonists. Reinitiation of anticoagulation was associated with a significantly lower risk of thromboembolic complications (pooled relative risk, 0.34; 95% confidence interval, 0.25-0.45; Q=5.12, P for heterogeneity=0.28). There was no evidence of increased risk of recurrent ICH after reinstatement of anticoagulation therapy, although there was significant heterogeneity among included studies (pooled relative risk, 1.01; 95% confidence interval, 0.58-1.77; Q=24.68, P for heterogeneity <0.001). No significant publication bias was detected in our analyses.
Conclusions: In observational studies, reinstitution of anticoagulation after ICH was associated with a lower risk of thromboembolic complications and a similar risk of ICH recurrence. Randomized clinical trials are needed to determine the true risk-benefit profile of anticoagulation resumption after ICH.
Keywords: anticoagulation; atrial fibrillation; myocardial infarction; stroke; thromboembolism.
© 2017 American Heart Association, Inc.
Conflict of interest statement
Figures
Comment in
-
Response by Murthy et al to Letter Regarding Article, "Restarting Anticoagulant Therapy After Intracranial Hemorrhage: A Systematic Review and Meta-Analysis".Stroke. 2017 Sep;48(9):e267. doi: 10.1161/STROKEAHA.117.018567. Epub 2017 Aug 7. Stroke. 2017. PMID: 28784921 Free PMC article. No abstract available.
-
Letter by Barco et al Regarding Article, "Restarting Anticoagulant Therapy After Intracranial Hemorrhage: A Systematic Review and Meta-Analysis".Stroke. 2017 Sep;48(9):e266. doi: 10.1161/STROKEAHA.117.018509. Epub 2017 Aug 7. Stroke. 2017. PMID: 28784924 No abstract available.
References
-
- Colilla S, Crow A, Petkun W, Singer DE, Simon T, Liu X. Estimates of current and future incidence and prevalence of atrial fibrillation in the u.S. Adult population. Am J Cardiol. 2013;112:1142–1147. - PubMed
-
- Hart RG, Pearce LA, Aguilar MI. Meta-analysis: Antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Annals of internal medicine. 2007;146:857–867. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, 3rd, Guyton RA, et al. 2014 aha/acc guideline for the management of patients with valvular heart disease: A report of the american college of cardiology/american heart association task force on practice guidelines. J Thorac Cardiovasc Surg. 2014;148:e1–e132. - PubMed
-
- Flaherty ML, Kissela B, Woo D, Kleindorfer D, Alwell K, Sekar P, et al. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology. 2007;68:116–121. - PubMed
-
- Garcia-Rodriguez LA, Gaist D, Morton J, Cookson C, Gonzalez-Perez A. Antithrombotic drugs and risk of hemorrhagic stroke in the general population. Neurology. 2013;81:566–574. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
