

The joint impact of cognitive performance in adolescence and familial cognitive aptitude on risk for major psychiatric disorders: a delineation of four potential pathways to illness
- PMID: 28416810
- PMCID: PMC5647225
- DOI: 10.1038/mp.2017.78
The joint impact of cognitive performance in adolescence and familial cognitive aptitude on risk for major psychiatric disorders: a delineation of four potential pathways to illness
Abstract
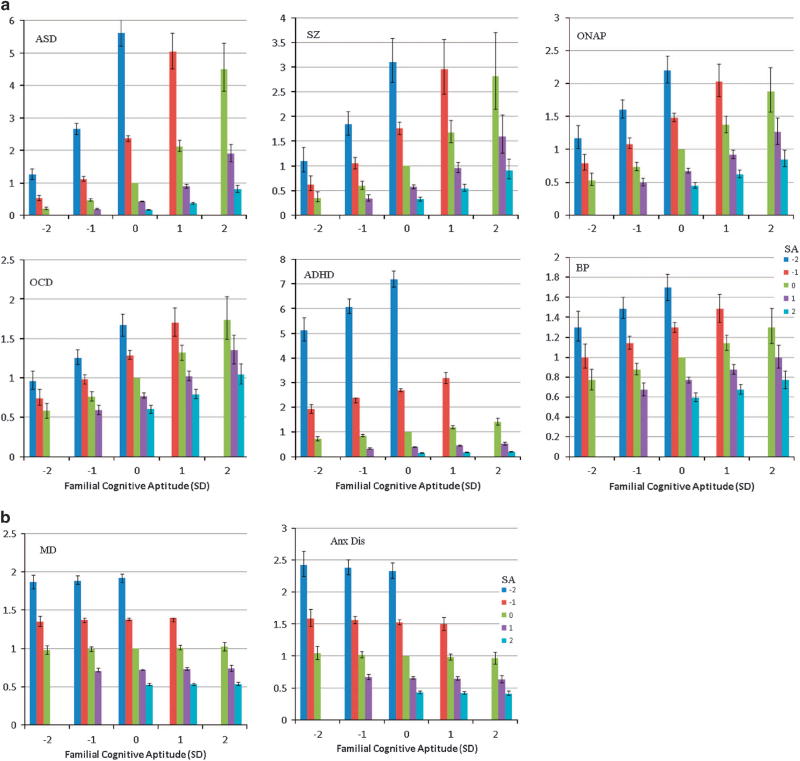
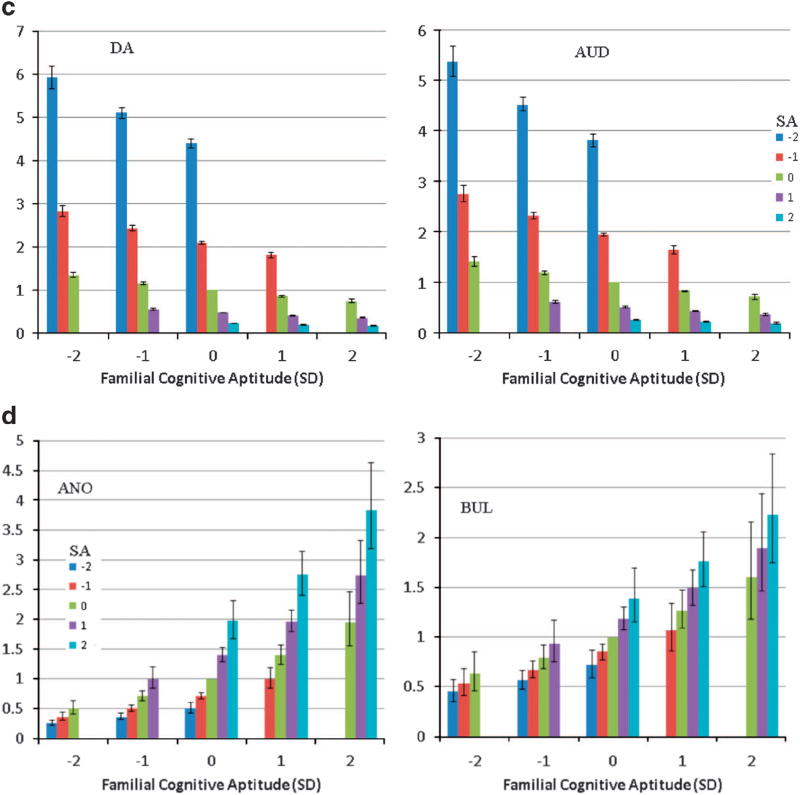
How do joint measures of premorbid cognitive ability and familial cognitive aptitude (FCA) reflect risk for a diversity of psychiatric and substance use disorders? To address this question, we examined, using Cox models, the predictive effects of school achievement (SA) measured at age 16 and FCA-assessed from SA in siblings and cousins, and educational attainment in parents-on risk for 12 major psychiatric syndromes in 1 140 608 Swedes born 1972-1990. Four developmental patterns emerged. In the first, risk was predicted jointly by low levels of SA and high levels of FCA-that is a level of SA lower than would be predicted from the FCA. This pattern was strongest in autism spectrum disorders and schizophrenia, and weakest in bipolar illness. In these disorders, a pathologic process seems to have caused cognitive functioning to fall substantially short of familial potential. In the second pattern, seen in the internalizing conditions of major depression and anxiety disorders, risk was associated with low SA but was unrelated to FCA. Externalizing disorders-drug abuse and alcohol use disorders-demonstrated the third pattern, in which risk was predicted jointly by low SA and low FCA. The fourth pattern, seen in eating disorders, was directly opposite of that observed in externalizing disorders with risk associated with high SA and high FCA. When measured together, adolescent cognitive ability and FCA identified four developmental patterns leading to diverse psychiatric disorders. The value of cognitive assessments in psychiatric research can be substantially increased by also evaluating familial cognitive potential.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Zammit S, Allebeck P, David AS, Dalman C, Hemmingsson T, Lundberg I, et al. A longitudinal study of premorbid IQ score and risk of developing schizophrenia, bipolar disorder, severe depression, and other nonaffective psychoses. Arch Gen Psychiatry. 2004;61:354–360. - PubMed
-
- Aylward E, Walker E, Bettes B. Intelligence in schizophrenia: meta-analysis of the research. Schizophr Bull. 1984;10:430–459. - PubMed
-
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance abuse prevention. Psychol Bull. 1992;112:64–105. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
