

Sentinel Lymph Node Biopsy: A new approach in the management of head and neck cancers
- PMID: 28417021
- PMCID: PMC5380418
- DOI: 10.18295/squmj.2016.17.01.002
Sentinel Lymph Node Biopsy: A new approach in the management of head and neck cancers
Abstract
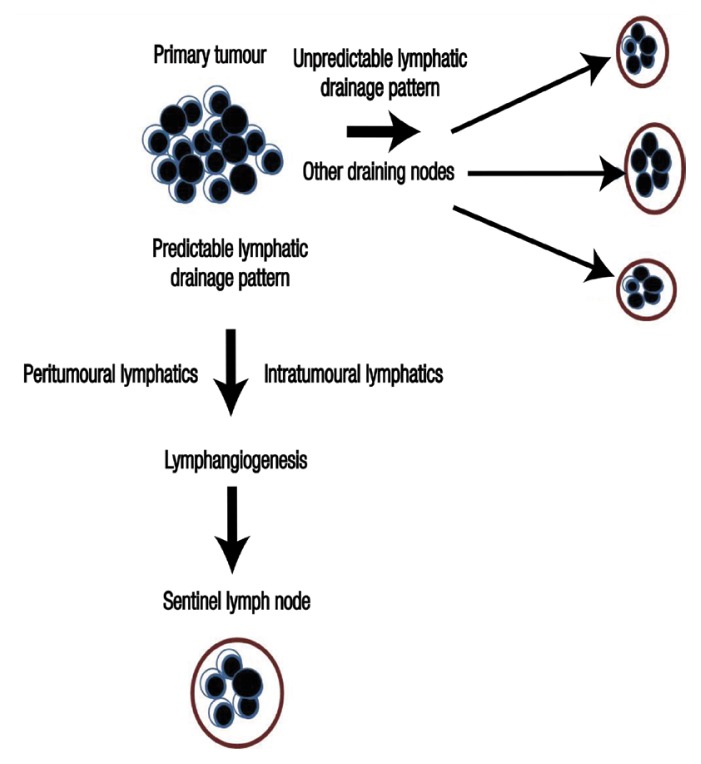
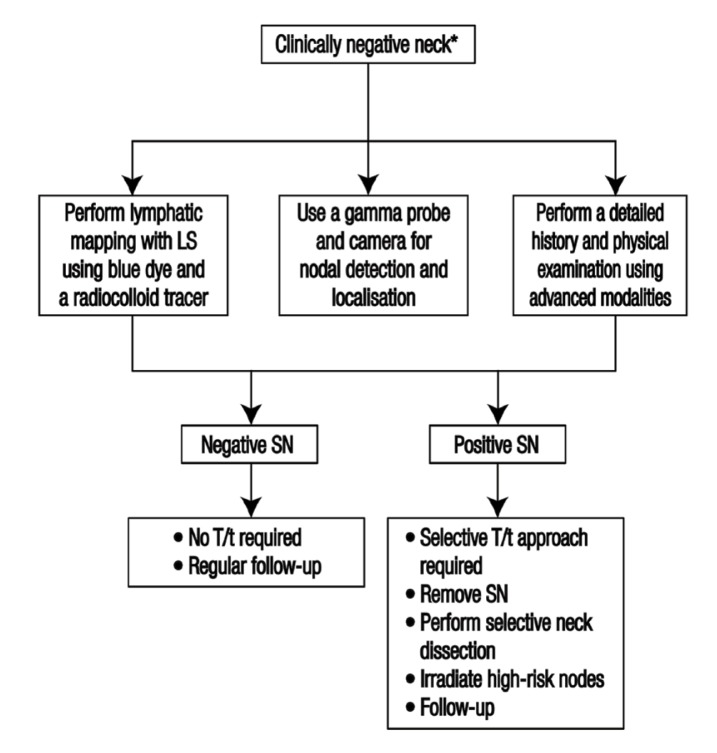
Cervical lymph node metastasis affects the prognosis and overall survival rate of and therapeutic planning for patients with head and neck squamous cell carcinomas (HNSCCs). However, advanced diagnostic modalities still lack accuracy in detecting occult neck metastasis. A sentinel lymph node biopsy is a minimally invasive auxiliary method for assessing the presence of occult metastatic disease in a patient with a clinically negative neck. This technique increases the specificity of neck dissection and thus reduces morbidity among oral cancer patients. The removal of sentinel nodes and dissection of the levels between the primary tumour and the sentinel node or the irradiation of target nodal basins is favoured as a selective treatment approach; this technique has the potential to become the new standard of care for patients with HNSCCs. This article presents an update on clinical applications and novel developments in this field.
Keywords: Head and Neck Cancer; Lymphoscintigraphy; Neck Dissection; Sentinel Lymph Node Biopsy; Squamous Cell Carcinomas.
Figures
Similar articles
-
Sentinel lymph node biopsy in head and neck squamous cell carcinoma.Laryngoscope. 2002 Dec;112(12):2101-13. doi: 10.1097/00005537-200212000-00001. Laryngoscope. 2002. PMID: 12461328
-
The use of sentinel node biopsy to upstage the clinically N0 neck in head and neck cancer.Arch Otolaryngol Head Neck Surg. 2002 Nov;128(11):1287-91. doi: 10.1001/archotol.128.11.1287. Arch Otolaryngol Head Neck Surg. 2002. PMID: 12431172
-
The application of sentinel node radiolocalization to solid tumors of the head and neck: a 10-year experience.Laryngoscope. 2004 Jan;114(1):2-19. doi: 10.1097/00005537-200401000-00002. Laryngoscope. 2004. PMID: 14709988 Review.
-
Elective neck dissection in oral carcinoma: a critical review of the evidence.Acta Otorhinolaryngol Ital. 2007 Jun;27(3):113-7. Acta Otorhinolaryngol Ital. 2007. PMID: 17883186 Free PMC article. Review.
-
Sentinel European Node Trial (SENT): 3-year results of sentinel node biopsy in oral cancer.Eur J Cancer. 2015 Dec;51(18):2777-84. doi: 10.1016/j.ejca.2015.08.023. Epub 2015 Nov 18. Eur J Cancer. 2015. PMID: 26597442
Cited by
-
Cervical metastasis of gingival carcinoma misdiagnosed as branchiogenic carcinoma, a rare entity - report of a case and review of literature.BMC Oral Health. 2017 Nov 28;17(1):139. doi: 10.1186/s12903-017-0435-9. BMC Oral Health. 2017. PMID: 29183323 Free PMC article. Review.
-
Artificial intelligence-driven radiomics study in cancer: the role of feature engineering and modeling.Mil Med Res. 2023 May 16;10(1):22. doi: 10.1186/s40779-023-00458-8. Mil Med Res. 2023. PMID: 37189155 Free PMC article. Review.
-
Current Approaches to Salvage Surgery for Head and Neck Cancer: A Comprehensive Review.Cancers (Basel). 2023 May 5;15(9):2625. doi: 10.3390/cancers15092625. Cancers (Basel). 2023. PMID: 37174091 Free PMC article. Review.
-
Head and neck cancer management and cancer stem cells implication.Saudi Dent J. 2019 Oct;31(4):395-416. doi: 10.1016/j.sdentj.2019.05.010. Epub 2019 Jun 10. Saudi Dent J. 2019. PMID: 31700218 Free PMC article. Review.
References
-
- Fidler IJ. Critical factors in the biology of human cancer metastasis: Twenty-eighth G.H.A. Clowes Memorial Award lecture. Cancer Res. 1990;50:6130–8. - PubMed
-
- Chen Z, Smith CW, Kiel D, Van Waes C. Metastatic variants derived following in vivo tumor progression of an in vitro transformed squamous cell carcinoma line acquire a differential growth advantage requiring tumor-host interaction. Clin Exp Metastasis. 1997;15:527–37. doi: 10.1023/A:1018474910432. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical