

Therapeutic CPAP Level Predicts Upper Airway Collapsibility in Patients With Obstructive Sleep Apnea
- PMID: 28419320
- PMCID: PMC6410952
- DOI: 10.1093/sleep/zsx056
Therapeutic CPAP Level Predicts Upper Airway Collapsibility in Patients With Obstructive Sleep Apnea
Abstract
Study objectives: Upper airway collapsibility is a key determinant of obstructive sleep apnea (OSA) which can influence the efficacy of certain non-continuous positive airway pressure (CPAP) treatments for OSA. However, there is no simple way to measure this variable clinically. The present study aimed to develop a clinically implementable tool to evaluate the collapsibility of a patient's upper airway.
Methods: Collapsibility, as characterized by the passive pharyngeal critical closing pressure (Pcrit), was measured in 46 patients with OSA. Associations were investigated between Pcrit and data extracted from patient history and routine polysomnography, including CPAP titration.
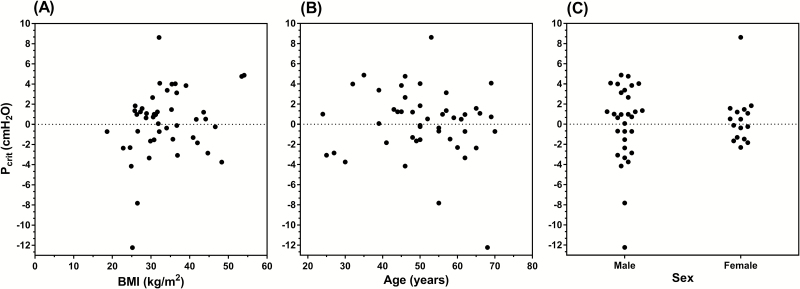
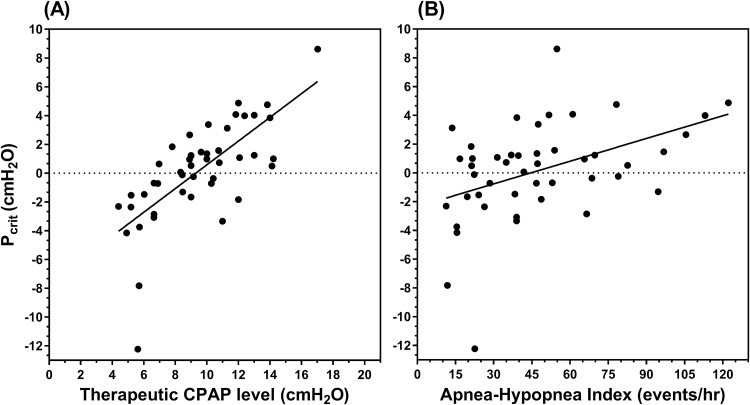
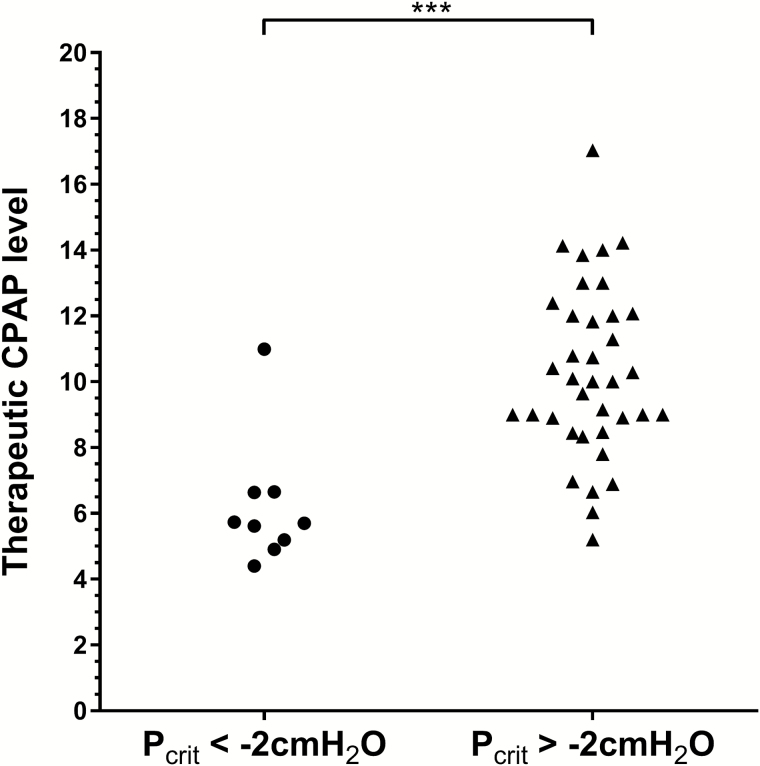
Results: Therapeutic CPAP level, demonstrated the strongest relationship to Pcrit (r2=0.51, p < .001) of all the variables investigated including apnea-hypopnea index, body mass index, sex, and age. Patients with a mildly collapsible upper airway (Pcrit ≤ -2 cmH2O) had a lower therapeutic CPAP level (6.2 ± 0.6 vs. 10.3 ± 0.4 cmH2O, p < .001) compared to patients with more severe collapsibility (Pcrit > -2 cmH2O). A therapeutic CPAP level ≤8.0 cmH2O was sensitive (89%) and specific (84%) for detecting a mildly collapsible upper airway. When applied to the independent validation data set (n = 74), this threshold maintained high specificity (91%) but reduced sensitivity (75%).
Conclusions: Our data demonstrate that a patient's therapeutic CPAP requirement shares a strong predictive relationship with their Pcrit and may be used to accurately differentiate OSA patients with mild airway collapsibility from those with moderate-to-severe collapsibility. Although this relationship needs to be confirmed prospectively, our findings may provide clinicians with better understanding of an individual patient's OSA phenotype, which ultimately could assist in determining which patients are most likely to respond to non-CPAP therapies.
Keywords: CPAP; Obstructive sleep apnea; Pcrit; collapsibility; phenotyping.
© Sleep Research Society 2017. Published by Oxford University Press on behalf of the Sleep Research Society. All rights reserved. For permissions, please e-mail journals.permissions@oup.com.
Figures
References
-
- Gleadhill IC, Schwartz AR, Schubert N, Wise RA, Permutt S, Smith PL. Upper airway collapsibility in snorers and in patients with obstructive hypopnea and apnea. Am Rev Respir Dis. 1991; 143(6): 1300–1303. - PubMed
-
- Younes M. Role of arousals in the pathogenesis of obstructive sleep apnea. Am J Respir Crit Care Med. 2004; 169(5): 623–633. - PubMed
