

Seizure Outcomes in Occipital Lobe and Posterior Quadrant Epilepsy Surgery: A Systematic Review and Meta-Analysis
- PMID: 28419330
- PMCID: PMC5640459
- DOI: 10.1093/neuros/nyx158
Seizure Outcomes in Occipital Lobe and Posterior Quadrant Epilepsy Surgery: A Systematic Review and Meta-Analysis
Abstract
Background: Occipital lobe epilepsy (OLE) is an uncommon but debilitating focal epilepsy syndrome with seizures often refractory to medical management. While surgical resection has proven a viable treatment, previous studies examining postoperative seizure freedom rates are limited by small sample size and patient heterogeneity, thus exhibiting significant variability in their results.
Objective: To review the medical literature on OLE so as to investigate rates and predictors of both seizure freedom and visual outcomes following surgery.
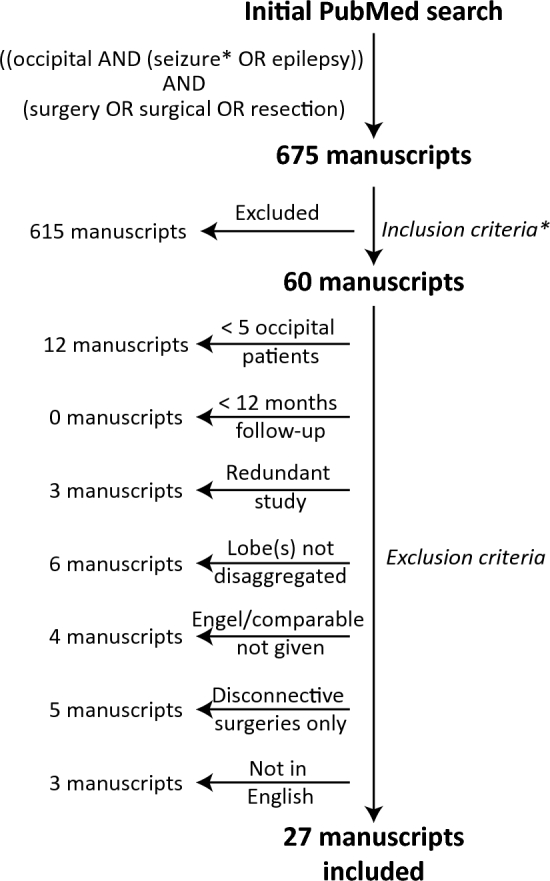
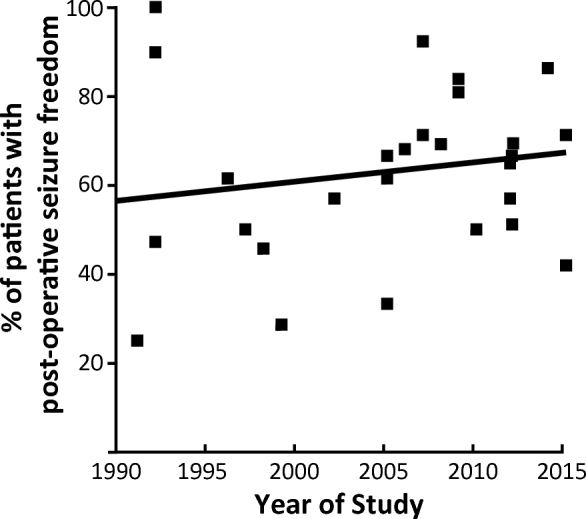
Methods: We reviewed manuscripts exploring surgical resection for drug-resistant OLE published between January 1990 and June 2015 on PubMed. Seizure freedom rates were analyzed and potential predictors were evaluated with separate meta-analyses. Postoperative visual outcomes were also examined.
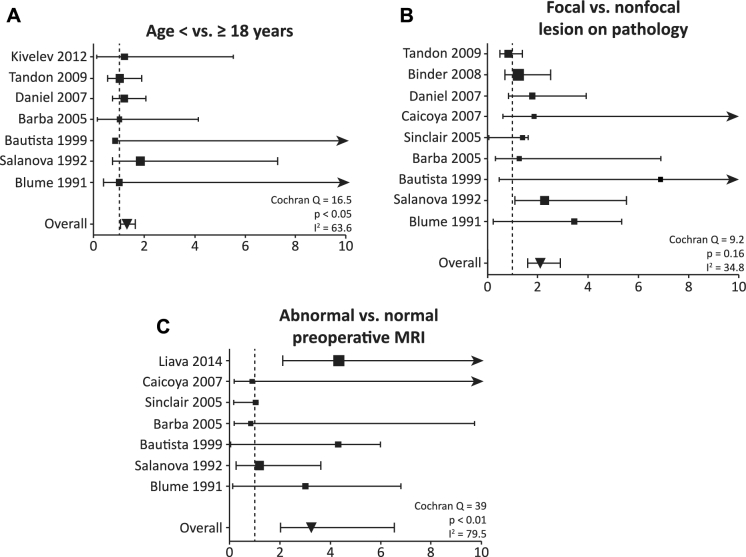
Results: We identified 27 case series comprising 584 patients with greater than 1 yr of follow-up. Postoperative seizure freedom (Engel class I outcome) was observed in 65% of patients, and was significantly predicted by age less than 18 yr (odds ratio [OR] 1.54, 95% confidence interval [CI] 1.13-2.18), focal lesion on pathological analysis (OR 2.08, 95% CI 1.58-2.89), and abnormal preoperative magnetic resonance imaging (OR 3.24, 95% 2.03-6.55). Of these patients, 175 also had visual outcomes reported with 57% demonstrating some degree of visual decline following surgery. We did not find any relationship between postoperative visual and seizure outcomes.
Conclusion: Surgical resection for OLE is associated with favorable outcomes with nearly two-thirds of patients achieving postoperative seizure freedom. However, patients must be counseled regarding the risk of visual decline following surgery.
Copyright © 2017 by the Congress of Neurological Surgeons
Figures
Comment in
-
Letter: Seizure Outcomes in Occipital Lobe and Posterior Quadrant Epilepsy Surgery: A Systematic Review and Meta-Analysis.Neurosurgery. 2019 Jun 1;84(6):E448. doi: 10.1093/neuros/nyz065. Neurosurgery. 2019. PMID: 30968133 No abstract available.
-
In Reply: Seizure Outcomes in Occipital Lobe and Posterior Quadrant Epilepsy Surgery: A Systematic Review and Meta-Analysis.Neurosurgery. 2019 Jun 1;84(6):E449. doi: 10.1093/neuros/nyz066. Neurosurgery. 2019. PMID: 30968144 No abstract available.
Similar articles
-
Occipital epilepsy: spatial categorization and surgical management.J Neurosurg. 2009 Feb;110(2):306-18. doi: 10.3171/2008.4.17490. J Neurosurg. 2009. PMID: 19046038
-
Surgical treatment of occipital lobe epilepsy.J Neurosurg. 2008 Jul;109(1):57-69. doi: 10.3171/JNS/2008/109/7/0057. J Neurosurg. 2008. PMID: 18590433
-
Resective Epilepsy Surgery for Tuberous Sclerosis in Children: Determining Predictors of Seizure Outcomes in a Multicenter Retrospective Cohort Study.Neurosurgery. 2015 Oct;77(4):517-24; discussion 524. doi: 10.1227/NEU.0000000000000875. Neurosurgery. 2015. PMID: 26120800
-
Patient phenotypes and clinical outcomes in invasive monitoring for epilepsy: An individual patient data meta-analysis.Epilepsy Behav. 2020 Jan;102:106652. doi: 10.1016/j.yebeh.2019.106652. Epub 2019 Nov 23. Epilepsy Behav. 2020. PMID: 31770717 Review.
-
Surgery for epilepsy.Cochrane Database Syst Rev. 2019 Jun 25;6(6):CD010541. doi: 10.1002/14651858.CD010541.pub3. Cochrane Database Syst Rev. 2019. PMID: 31237346 Free PMC article.
Cited by
-
Changes in Functional Connectivity of Specific Cerebral Regions in Patients with Toothache: A Resting-State Functional Magnetic Resonance Imaging Study.Dis Markers. 2020 Dec 28;2020:6683161. doi: 10.1155/2020/6683161. eCollection 2020. Dis Markers. 2020. PMID: 33456630 Free PMC article.
-
Occipital lobe epilepsy surgery: treating seizures in the posterior cortex.Neurosurg Rev. 2024 Aug 30;47(1):514. doi: 10.1007/s10143-024-02772-8. Neurosurg Rev. 2024. PMID: 39212792 Review.
-
Prognostic value of ictal onset patterns in postsurgical outcome of temporal lobe epilepsy.Iran J Neurol. 2017 Oct 7;16(4):185-191. Iran J Neurol. 2017. PMID: 29736224 Free PMC article.
-
Getting the best outcomes from epilepsy surgery.Ann Neurol. 2018 Apr;83(4):676-690. doi: 10.1002/ana.25205. Epub 2018 Apr 10. Ann Neurol. 2018. PMID: 29534299 Free PMC article. Review.
-
Comparative Effectiveness of Stereotactic Electroencephalography Versus Subdural Grids in Epilepsy Surgery.Ann Neurol. 2021 Dec;90(6):927-939. doi: 10.1002/ana.26238. Epub 2021 Oct 14. Ann Neurol. 2021. PMID: 34590337 Free PMC article.
References
-
- Taylor I, Scheffer IE, Berkovic SF. Occipital epilepsies: identification of specific and newly recognized syndromes. Brain. 2003;126(pt 4):753-769. - PubMed
-
- Manford M, Hart YM, Sander JW, Shorvon SD. National general practice study of epilepsy (NGPSE): partial seizure patterns in a general population. Neurology. 1992;42(10):1911-1917. - PubMed
-
- Tandon N, Alexopoulos AV, Warbel A, Najm IM, Bingaman WE. Occipital epilepsy: spatial categorization and surgical management. J Neurosurg. 2009;110(2):306-318. - PubMed
-
- Williamson PD, Thadani VM, Darcey TM, Spencer DD, Spencer SS, Mattson RH. Occipital lobe epilepsy: clinical characteristics, seizure spread patterns, and results of surgery. Ann Neurol. 1992;31(1):3-13. - PubMed
-
- Aykut-Bingol C, Bronen RA, Kim JH, Spencer DD, Spencer SS. Surgical outcome in occipital lobe epilepsy: implications for pathophysiology. Ann Neurol. 1998;44(1):60-69. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
