

The role of stromal cells in inflammatory bone loss
- PMID: 28419440
- PMCID: PMC5461090
- DOI: 10.1111/cei.12979
The role of stromal cells in inflammatory bone loss
Abstract
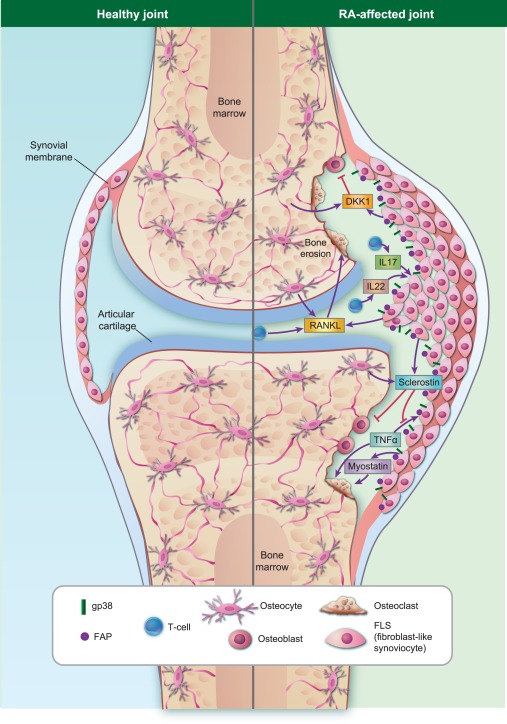
Rheumatoid arthritis (RA) is an autoimmune disease characterized by chronic inflammation, local and systemic bone loss and a lack of compensatory bone repair. Fibroblast-like synoviocytes (FLS) are the most abundant cells of the stroma and a key population in autoimmune diseases such as RA. An increasing body of evidence suggests that these cells play not only an important role in chronic inflammation and synovial hyperplasia, but also impact bone remodelling. Under inflammatory conditions FLS release inflammatory cytokines, regulate bone destruction and formation and communicate with immune cells to control bone homeostasis. Other stromal cells, such as osteoblasts and terminally differentiated osteoblasts, termed osteocytes, are also involved in the regulation of bone homeostasis and are dysregulated during inflammation. This review highlights our current understanding of how stromal cells influence the balance between bone formation and bone destruction. Increasing our understanding of these processes is critical to enable the development of novel therapeutic strategies with which to treat bone loss in RA.
Keywords: RA; RA-FLS; bone remodelling; inflammatory cytokines; stromal cells.
© 2017 British Society for Immunology.
Figures
References
-
- Tak PP, Bresnihan B. The pathogenesis and prevention of joint damage in rheumatoid arthritis: advances from synovial biopsy and tissue analysis. Arthritis Rheum 2000; 43:2619–33. - PubMed
-
- Korb‐Pap A, Bertrand J, Sherwood J, Pap T. Stable activation of fibroblasts in rheumatic arthritis – causes and consequences. Rheumatology (Oxford) 2016; 55:ii64–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
