

Cardiorespiratory physiology in the safe passage study: protocol, methods and normative values in unexposed infants
- PMID: 28419567
- PMCID: PMC5530586
- DOI: 10.1111/apa.13873
Cardiorespiratory physiology in the safe passage study: protocol, methods and normative values in unexposed infants
Abstract
Aim: The Safe Passage Study, conducted by the Prenatal Alcohol in SIDS and Stillbirth Network, is investigating contributions of prenatal alcohol exposure to foetal and infant demise. This current report presents physiological data from full-term infants with no prenatal exposure to alcohol or maternal smoking.
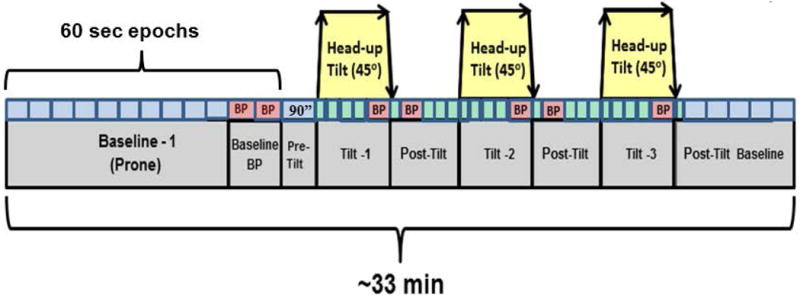
Methods: Data are from 666 infants from the Northern Plains (North and South Dakota) and South Africa. A standardised protocol assessed cardiorespiratory function during baseline and head-up tilts shortly after birth and at one month of age.
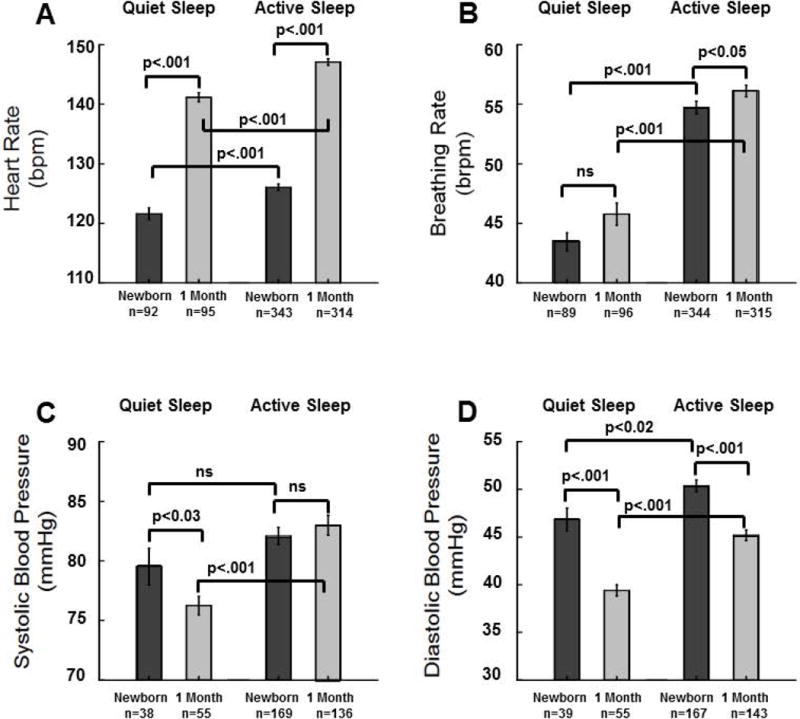
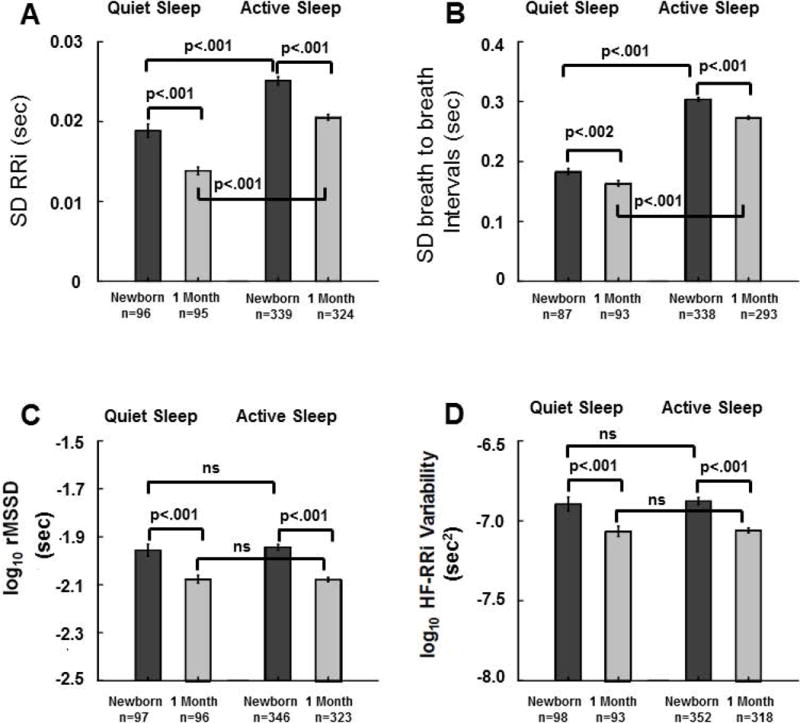
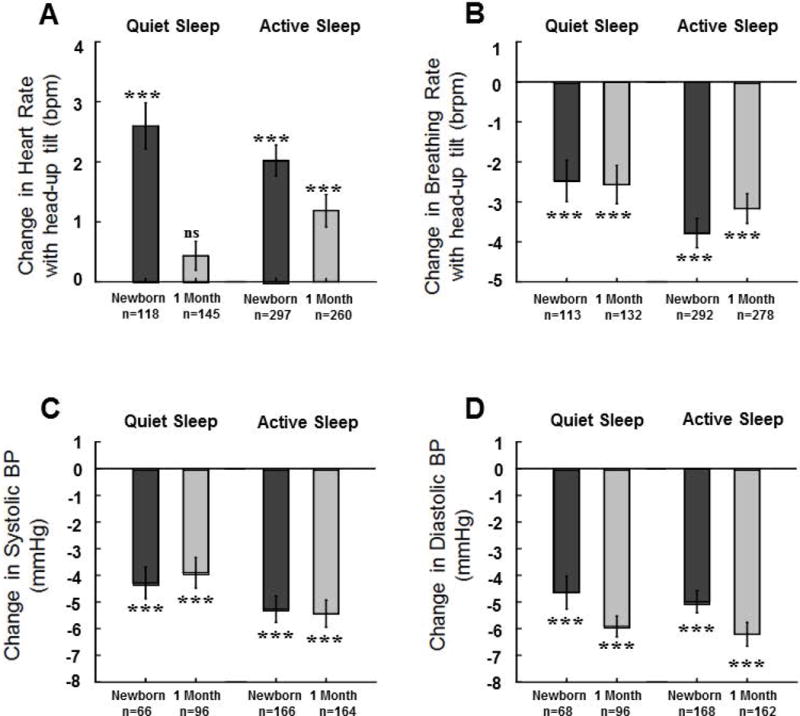
Results: Analyses revealed significant increases in heart rate and decreases in BP from the newborn to one-month time period as well as diminished heart rate responses to head-up tilt in one-month-old infants.
Conclusion: The Safe Passage Study was successful in characterising physiology in a large number of infants at sites known to have elevated risks for SIDS. Results demonstrate that even with low prenatal adverse exposures, there are significant changes in cardiorespiratory function as infants enter the window of increased risk for SIDS.
Keywords: SIDS; Autonomic development; Blood pressure; Heart rate; Respiration.
©2017 Foundation Acta Paediatrica. Published by John Wiley & Sons Ltd.
Conflict of interest statement
Figures

References
-
- Carlin RF, Moon RY. Risk Factors, Protective Factors, and Current Recommendations to Reduce Sudden Infant Death Syndrome: A Review. JAMA Pediatr. 2017;171:175–80. - PubMed
-
- Franco P, Lipshut W, Valente F, Adams S, Groswasser J, Kahn A. Cardiac autonomic characteristics in infants sleeping with their head covered by bedclothes. J Sleep Res. 2003;12:125–32. - PubMed
-
- Horne RS, Parslow PM, Harding R. Respiratory control and arousal in sleeping infants. Paediatr Respir Rev. 2004;5:190–8. - PubMed
-
- Horne RS, Witcombe NB, Yiallourou SR, Scaillet S, Thiriez G, Franco P. Cardiovascular control during sleep in infants: Implications for Sudden Infant Death Syndrome. Sleep Med. 2010;11:615–21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
