

Leydig cell tumor in grey zone: A case report
- PMID: 28419904
- PMCID: PMC5394201
- DOI: 10.1016/j.ijscr.2017.03.043
Leydig cell tumor in grey zone: A case report
Abstract
Introduction: Leydig cell tumor constitutes only about 1-3% of testicular neoplasms. There is apparently increased incidence in the last few years; one possible explanation for this phenomenon is the widespread use of ultrasound technology and the subsequent increased early detection of smaller lesions that have not been found in historical series.
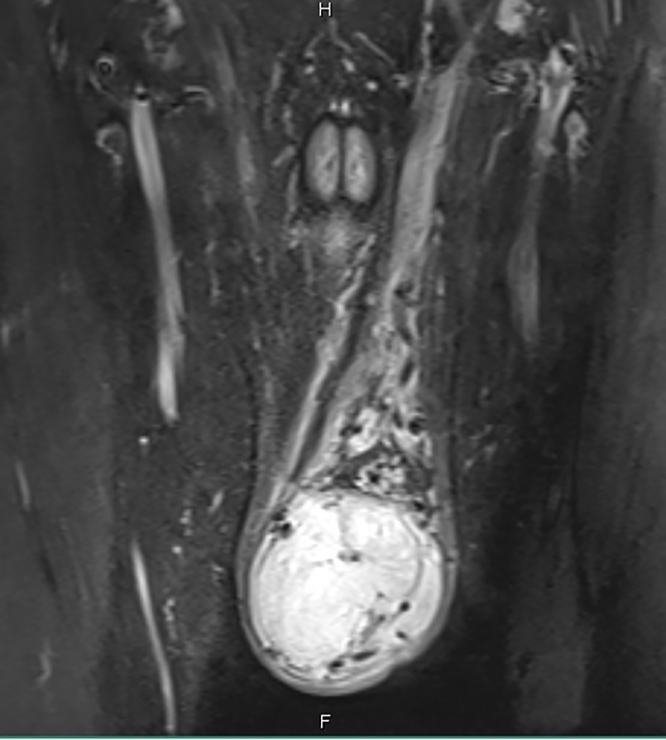
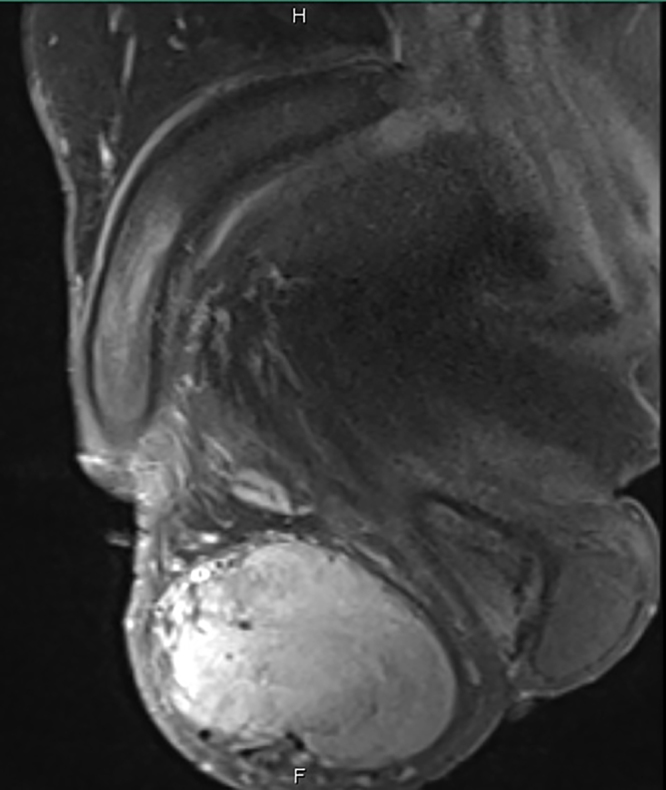
Case presentation: We report a case of Leydig cell tumor of testis in a patient presenting with painless long standing slowly growing left scrotal mass who found to have intrapulmonary nodule and multiple enlarged retroperitoneal lymph nodes on staging work up. The mass was managed by radical orchiectomy. Pathological diagnosis was Leydig cell tumor.
Discussion: Orchiectomy is the accepted mode of treatment but follow-up every 3-6 months with physical examination, hormone assays, scrotal and abdominal ultrasonography, chest radiography, and CT scans is essential in such a case with a potential for malignant behavior.
Conclusion: Inguinal orchiectomy is the therapeutic decision of choice and long-term follow-up is necessary to exclude recurrence or metastasis. Cases which fall in the grey zone like ours need to be followed up carefully for metastasis instead of rushing into an early retroperitoneal lymph node dissection, with its potential risks and complications.
Keywords: Inguinal orchiectomy; Leydig cell tumor; Malignant behavior; RPLND; Testicular neoplasms.
Copyright © 2017 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures









Similar articles
-
Testicular tumors in children.J Pediatr Surg. 2001 Dec;36(12):1796-801. doi: 10.1053/jpsu.2001.28841. J Pediatr Surg. 2001. PMID: 11733909
-
Long-term follow-up using testicle-sparing surgery for Leydig cell tumor.Clin Genitourin Cancer. 2013 Sep;11(3):321-4. doi: 10.1016/j.clgc.2012.12.008. Epub 2013 Jan 11. Clin Genitourin Cancer. 2013. PMID: 23317518
-
Conservative surgical therapy for leydig cell tumor.J Urol. 2007 Aug;178(2):507-11; discussion 511. doi: 10.1016/j.juro.2007.03.108. Epub 2007 Jun 11. J Urol. 2007. PMID: 17561156
-
[A case of testicular tumor associated with the contralateral undescended testis].Hinyokika Kiyo. 1995 Dec;41(12):1015-8. Hinyokika Kiyo. 1995. PMID: 8578983 Review. Japanese.
-
Current controversies on the role of retroperitoneal lymphadenectomy for testicular cancer.Urol Oncol. 2019 Mar;37(3):209-218. doi: 10.1016/j.urolonc.2018.09.009. Epub 2018 Nov 13. Urol Oncol. 2019. PMID: 30446455 Free PMC article. Review.
Cited by
-
Unilateral pubic hair growth: a paracrine finding indicative of underlying leydig cell tumor in a prepubertal boy.Urol Case Rep. 2025 May 17;61:103071. doi: 10.1016/j.eucr.2025.103071. eCollection 2025 Jul. Urol Case Rep. 2025. PMID: 40496178 Free PMC article.
-
Testicular Vein Sampling Can Reveal Gonadotropin-Independent Unilateral Steroidogenesis Supporting Spermatogenesis.J Endocr Soc. 2019 Jul 30;3(10):1881-1886. doi: 10.1210/js.2019-00180. eCollection 2019 Oct 1. J Endocr Soc. 2019. PMID: 31592497 Free PMC article.
-
Loss of libido in a man with an incidental Leydig cell tumour of the testis: a rare tumour discovered following an isolated common complaint.J Surg Case Rep. 2020 Jul 16;2020(7):rjaa241. doi: 10.1093/jscr/rjaa241. eCollection 2020 Jul. J Surg Case Rep. 2020. PMID: 33343871 Free PMC article.
-
Management of testicular Leydig cell tumor: A case report.Medicine (Baltimore). 2018 Jun;97(25):e11158. doi: 10.1097/MD.0000000000011158. Medicine (Baltimore). 2018. PMID: 29924022 Free PMC article.
-
Testicular leydig cell tumor revealed by hydrocele.Urol Case Rep. 2020 Dec 5;35:101520. doi: 10.1016/j.eucr.2020.101520. eCollection 2021 Mar. Urol Case Rep. 2020. PMID: 33318945 Free PMC article.
References
-
- Agha R.A., Fowler A.J., Saetta A., Barai I., Rajmohan S., Orgill D.P., the SCARE Group The SCARE statement: consensus-based surgical case report guidelines. Int. J. Surg. 2016;34:180–186. - PubMed
-
- Tichoo S.K., Tamboli P., Warner N.E., Amin M.B. Testicular and paratesticular tumors. In: Weidner N., Cote R.J., Suster S., Weiss L.M., editors. Modern Surgical Pathology. Elsevier Science; Philadelphia: Saunders: 2003. pp. 1215–1256.
-
- Kim I., Young R.H., Scully R.E. Leydig cell tumors of the testis: a clinicopathological analysis of 40 casesand review of the literature. Am. J. Surg. Pathol. 1985;9:177–192. - PubMed
-
- Henderson C.G., Ahmed A.A., Sesterhenn I. Enucleation for prepubertal Leydig cell tumor. J. Urol. 2006;176:703–705. - PubMed
-
- Sugimoto K., Matsumoto S., Nose K. A malignant Leydig cell tumor of the testis. Int. Urol. Nephrol. 2006;38:291–292. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
