

Cerebral Autoregulation, Brain Injury, and the Transitioning Premature Infant
- PMID: 28421173
- PMCID: PMC5377300
- DOI: 10.3389/fped.2017.00064
Cerebral Autoregulation, Brain Injury, and the Transitioning Premature Infant
Abstract
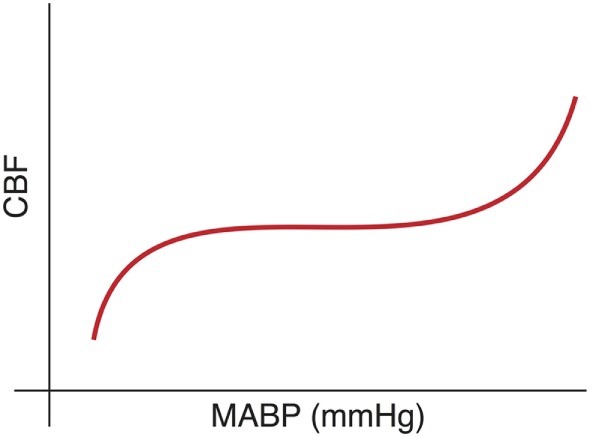
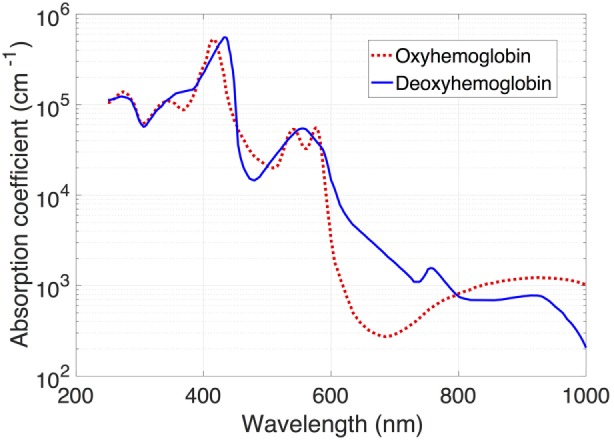
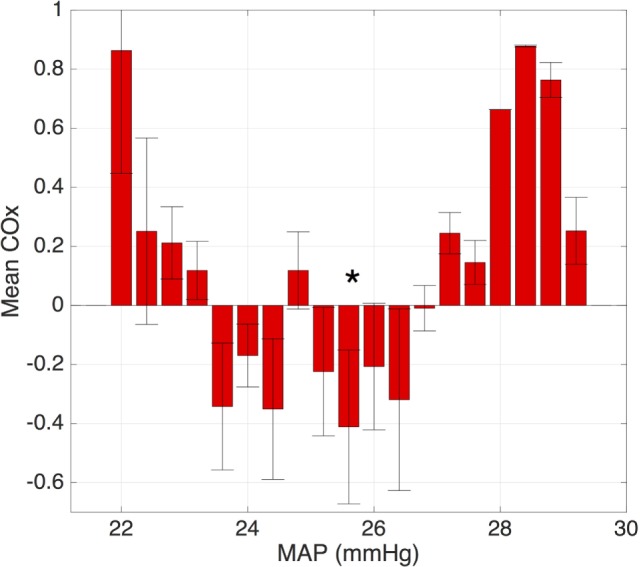
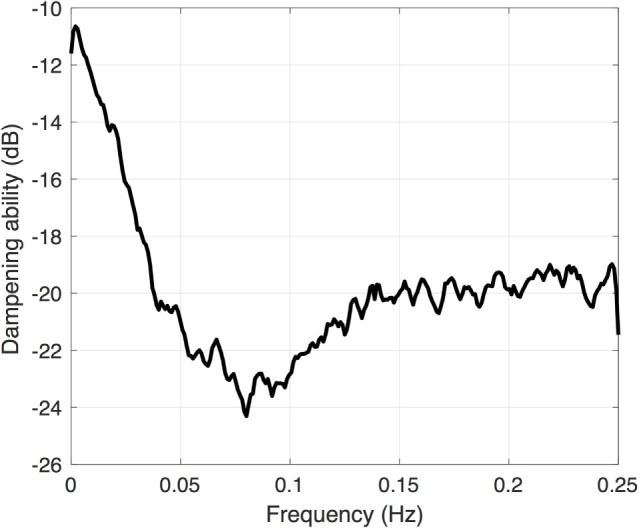
Improvements in clinical management of the preterm infant have reduced the rates of the two most common forms of brain injury, such as severe intraventricular hemorrhage and white matter injury, both of which are contributory factors in the development of cerebral palsy. Nonetheless, they remain a persistent challenge and are associated with a significant increase in the risk of adverse neurodevelopment outcomes. Repeated episodes of ischemia-reperfusion represent a common pathway for both forms of injury, arising from discordance between systemic blood flow and the innate regulation of cerebral blood flow in the germinal matrix and periventricular white matter. Nevertheless, establishing firm hemodynamic boundaries, as a part of neuroprotective strategy, has challenged researchers. Existing measures either demonstrate inconsistent relationships with injury, as in the case of mean arterial blood pressure, or are not feasible for long-term monitoring, such as cardiac output estimated by echocardiography. These challenges have led some researchers to focus on the mechanisms that control blood flow to the brain, known as cerebrovascular autoregulation. Historically, the function of the cerebrovascular autoregulatory system has been difficult to quantify; however, the evolution of bedside monitoring devices, particularly near-infrared spectroscopy, has enabled new insights into these mechanisms and how impairment of blood flow regulation may contribute to catastrophic injury. In this review, we first seek to examine how technological advancement has changed the assessment of cerebrovascular autoregulation in premature infants. Next, we explore how clinical factors, including hypotension, vasoactive medications, acute and chronic hypoxia, and ventilation, alter the hemodynamic state of the preterm infant. Additionally, we examine how developmentally linked or acquired dysfunction in cerebral autoregulation contributes to preterm brain injury. In conclusion, we address exciting new approaches to the measurement of autoregulation and discuss the feasibility of translation to the bedside.
Keywords: autoregulation; brain injury; intraventricular hemorrhage; near-infrared spectroscopy; prematurity; white matter injury.
Figures
References
-
- Stevenson DK, Wright LL, Lemons JA, Oh W, Korones SB, Papile LA, et al. Very low birth weight outcomes of the National Institute of Child Health and Human Development Neonatal Research Network, January 1993 through December 1994. Am J Obstet Gynecol (1998) 179:1632–9.10.1016/S0002-9378(98)70037-7 - DOI - PubMed
-
- Volpe JJ. Neurology of the Newborn. 5th ed Philadelphia: Saunders/Elsevier; (2008).
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical