

Long-Term Testosterone Therapy Improves Cardiometabolic Function and Reduces Risk of Cardiovascular Disease in Men with Hypogonadism: A Real-Life Observational Registry Study Setting Comparing Treated and Untreated (Control) Groups
- PMID: 28421834
- PMCID: PMC5555449
- DOI: 10.1177/1074248417691136
Long-Term Testosterone Therapy Improves Cardiometabolic Function and Reduces Risk of Cardiovascular Disease in Men with Hypogonadism: A Real-Life Observational Registry Study Setting Comparing Treated and Untreated (Control) Groups
Abstract
Objectives: In the absence of large, prospective, placebo-controlled studies of longer duration, substantial evidence regarding the safety and risk of testosterone (T) therapy (TTh) with regard to cardiovascular (CV) outcomes can only be gleaned from observational studies. To date, there are limited studies comparing the effects of long-term TTh in men with hypogonadism who were treated or remained untreated with T, for obvious reasons. We have established a registry to assess the long-term effectiveness and safety of T in men in a urological setting. Here, we sought to compare the effects of T on a host of parameters considered to contribute to CV risk in treated and untreated men with hypogonadism (control group).
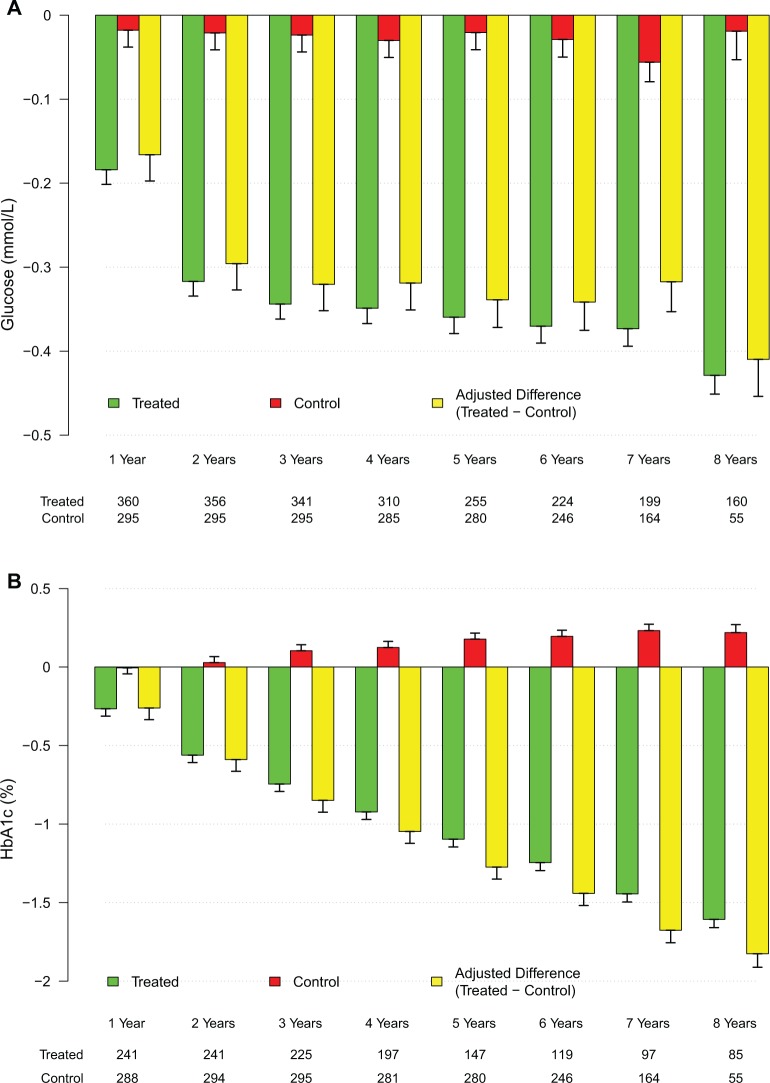
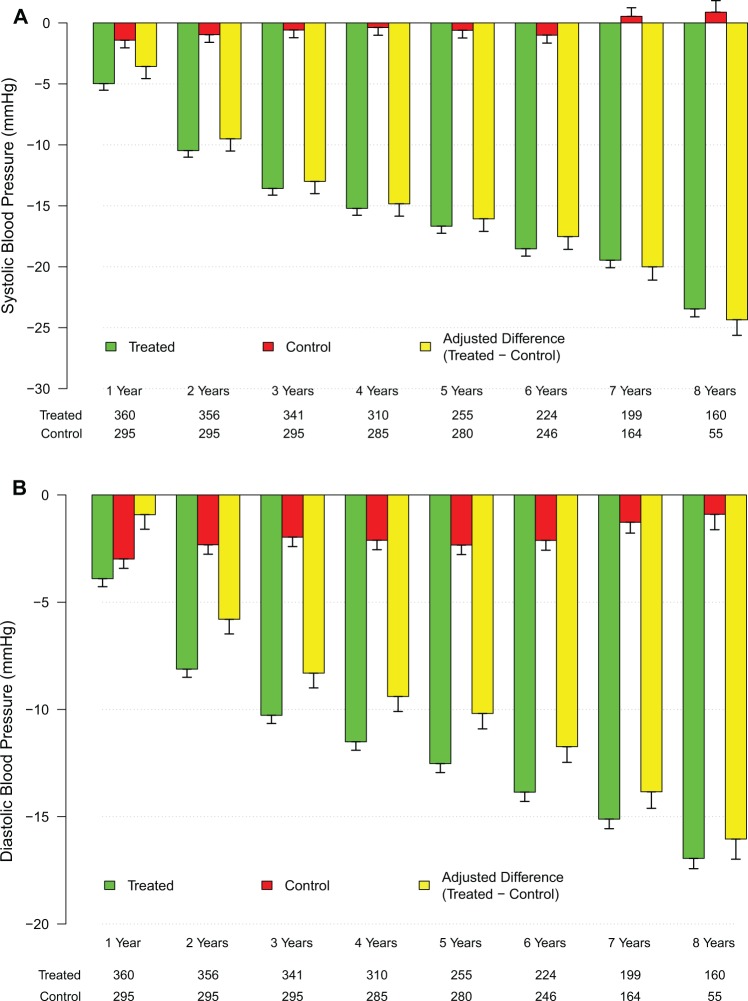
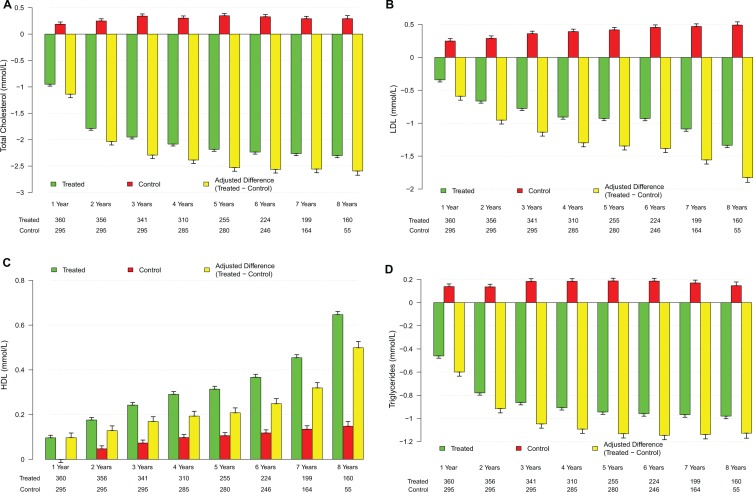
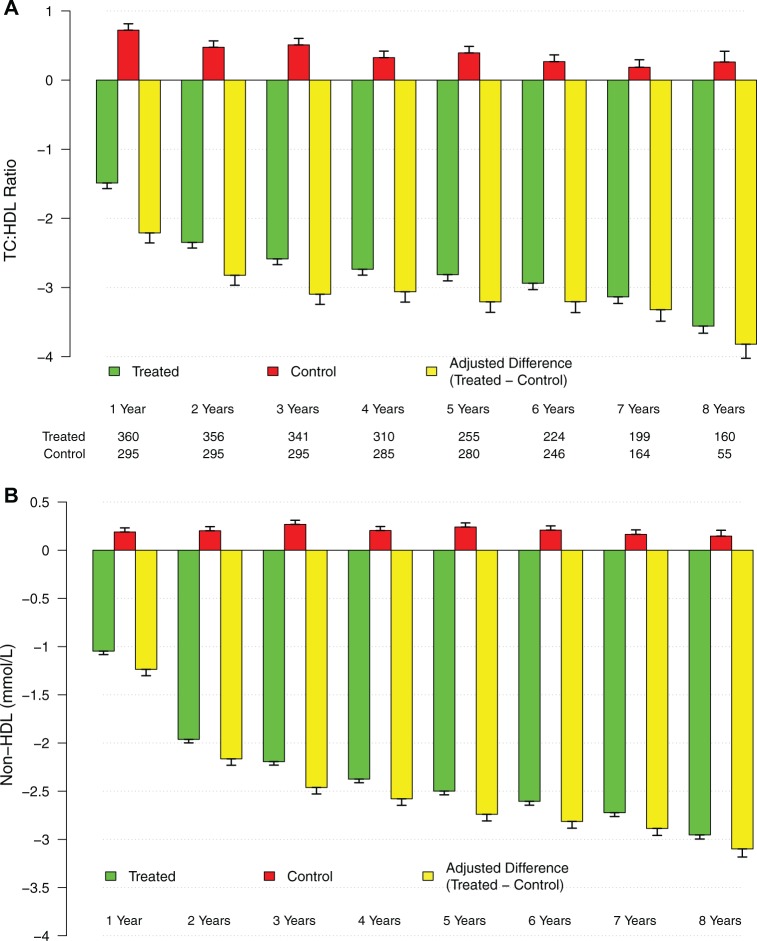
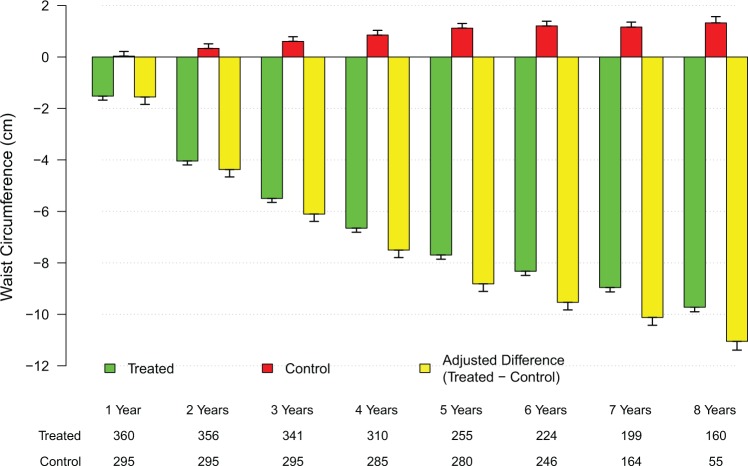
Patients and methods: Observational, prospective, cumulative registry study in 656 men (age: 60.7 ± 7.2 years) with total T levels ≤12.1 nmol/L and symptoms of hypogonadism. In the treatment group, men (n = 360) received parenteral T undecanoate (TU) 1000 mg/12 weeks following an initial 6-week interval for up to 10 years. Men (n = 296) who had opted against TTh served as controls. Median follow-up in both groups was 7 years. Measurements were taken at least twice a year, and 8-year data were analyzed. Mean changes over time between the 2 groups were compared by means of a mixed-effects model for repeated measures, with a random effect for intercept and fixed effects for time, group, and their interaction. To account for baseline differences between the 2 groups, changes were adjusted for age, weight, waist circumference, fasting glucose, blood pressure, and lipids.
Results: There were 2 deaths in the T-treated group, none was related to CV events. There were 21 deaths in the untreated (control) group, 19 of which were related to CV events. The incidence of death in 10 patient-years was 0.1145 in the control group (95% confidence interval [CI]: 0.0746-0.1756; P < .000) and 0.0092 in the T-treated group (95% CI: 0.0023-0.0368; P < .000); the estimated difference between groups was 0.0804 (95% CI: 0.0189-0.3431; P < .001). The estimated reduction in mortality for the T-group was between 66% and 92%. There were also 30 nonfatal strokes and 26 nonfatal myocardial infarctions in the control group and none in the T-treated group.
Conclusion: Long-term TU was well tolerated with excellent adherence suggesting a high level of patient satisfaction. Mortality related to CV disease was significantly reduced in the T-group.
Keywords: anthropometric parameters; cardiometabolic function; cardiovascular risk; hypogonadism; mortality; testosterone.
Conflict of interest statement
Figures
Similar articles
-
Hypogonadal men with moderate-to-severe lower urinary tract symptoms have a more severe cardiometabolic risk profile and benefit more from testosterone therapy than men with mild lower urinary tract symptoms.Investig Clin Urol. 2018 Nov;59(6):399-409. doi: 10.4111/icu.2018.59.6.399. Epub 2018 Nov 2. Investig Clin Urol. 2018. PMID: 30402573 Free PMC article.
-
Differential effects of 11 years of long-term injectable testosterone undecanoate therapy on anthropometric and metabolic parameters in hypogonadal men with normal weight, overweight and obesity in comparison with untreated controls: real-world data from a controlled registry study.Int J Obes (Lond). 2020 Jun;44(6):1264-1278. doi: 10.1038/s41366-019-0517-7. Epub 2020 Jan 28. Int J Obes (Lond). 2020. PMID: 32060355 Free PMC article.
-
Men with testosterone deficiency and a history of cardiovascular diseases benefit from long-term testosterone therapy: observational, real-life data from a registry study.Vasc Health Risk Manag. 2016 Jun 14;12:251-61. doi: 10.2147/VHRM.S108947. eCollection 2016. Vasc Health Risk Manag. 2016. PMID: 27366080 Free PMC article.
-
Cardiovascular Morbidity and Mortality in Men - Findings From a Meta-analysis on the Time-related Measure of Risk of Exogenous Testosterone.J Sex Med. 2022 Aug;19(8):1243-1254. doi: 10.1016/j.jsxm.2022.05.145. Epub 2022 Jun 23. J Sex Med. 2022. PMID: 35753891 Review.
-
Testosterone and Cardiovascular Risk: Meta-Analysis of Interventional Studies.J Sex Med. 2018 Jun;15(6):820-838. doi: 10.1016/j.jsxm.2018.04.641. J Sex Med. 2018. PMID: 29803351 Review.
Cited by
-
Understanding Erectile Dysfunction in Hypertensive Patients: The Need for Good Patient Management.Vasc Health Risk Manag. 2020 Jun 12;16:231-239. doi: 10.2147/VHRM.S223331. eCollection 2020. Vasc Health Risk Manag. 2020. PMID: 32606719 Free PMC article. Review.
-
The role of sex differences in cardiovascular, metabolic, and immune functions in health and disease: a review for "Sex Differences in Health Awareness Day".Biol Sex Differ. 2025 May 13;16(1):33. doi: 10.1186/s13293-025-00714-7. Biol Sex Differ. 2025. PMID: 40361226 Free PMC article. Review.
-
Androgen-Regulated Cardiac Metabolism in Aging Men.Front Endocrinol (Lausanne). 2020 May 15;11:316. doi: 10.3389/fendo.2020.00316. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32499759 Free PMC article. Review.
-
Testosterone and the Heart.Eur Cardiol. 2019 Jul 11;14(2):103-110. doi: 10.15420/ecr.2019.13.1. eCollection 2019 Jul. Eur Cardiol. 2019. PMID: 31360231 Free PMC article. Review.
-
Emerging Evidences in the Long Standing Controversy Regarding Testosterone Replacement Therapy and Cardiovascular Events.World J Mens Health. 2018 May;36(2):92-102. doi: 10.5534/wjmh.17050. World J Mens Health. 2018. PMID: 29706034 Free PMC article. Review.
References
-
- Traish AM, Zitzmann M. The complex and multifactorial relationship between testosterone deficiency (TD), obesity and vascular disease. Rev Endocr Metab Disord. 2015;16(3):249–268. - PubMed
-
- Traish AM. Adverse health effects of testosterone deficiency (TD) in men. Steroids. 2014;88:106–116. - PubMed
-
- Kelly DM, Jones TH. Testosterone and obesity. Obes Rev. 2015;16(7):581–606. - PubMed
-
- Traish AM. Outcomes of testosterone therapy in men with testosterone deficiency (TD): part II. Steroids. 2014;88:117–126. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
