

Adult-onset cystic fibrosis liver disease: Diagnosis and characterization of an underappreciated entity
- PMID: 28422310
- PMCID: PMC5519421
- DOI: 10.1002/hep.29217
Adult-onset cystic fibrosis liver disease: Diagnosis and characterization of an underappreciated entity
Abstract
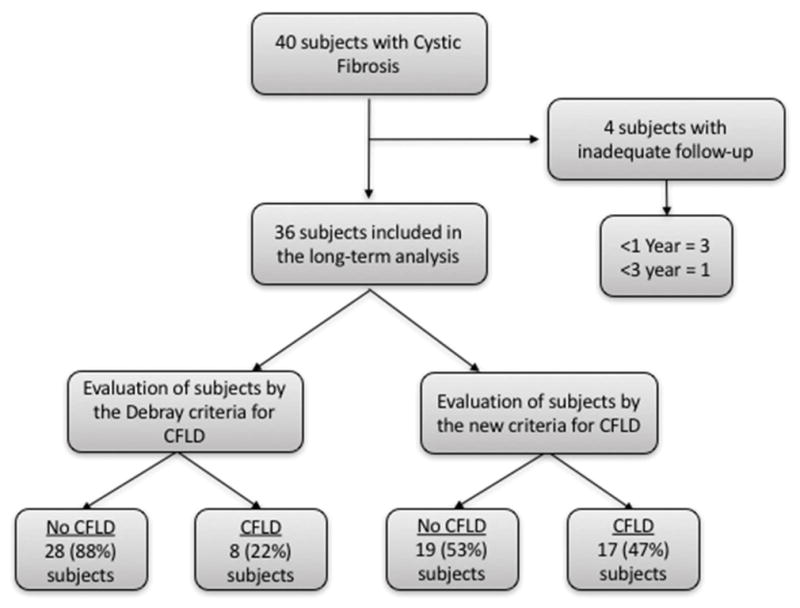
Cystic fibrosis (CF) liver disease (CFLD), a leading cause of death in CF, is mostly described in pediatric populations. Adult-onset CFLD lacks sufficient characterization and diagnostic tools. A cohort of CF patients without CFLD during childhood were followed for up to 38 years with serologic testing, imaging, and noninvasive fibrosis markers. Historical CFLD diagnostic criteria were compared with newly proposed CFLD criteria. Thirty-six CF patients were followed for a median of 24.5 years (interquartile range 15.6-32.9). By the last follow-up, 11 (31%) had died. With conventional criteria, 8 (22%) patients had CFLD; and by the new criteria, 17 (47%) had CFLD at a median age of 36.6 years (interquartile range 26.5-43.2). By the new criteria, those with CFLD had higher median alanine aminotransferase (42 versus 27, P = 0.005), aspartate aminotransferase (AST; 26 versus 21, P = 0.01), direct bilirubin (0.13 versus 0.1, P = 0.01), prothrombin time (14.4 versus 12.4, P = 0.002), and AST-to-platelet ratio index (0.31 versus 0.23, P = 0.003) over the last 2 years of follow-up. Subjects with a FibroScan >6.8 kPa had higher alanine aminotransferase (42 versus 28U/L, P = 0.02), AST (35 versus 25U/L, P = 0.02), AST-to-platelet ratio index (0.77 versus 0.25, P = 0.0004), and Fibrosis-4 index (2.14 versus 0.74, P = 0.0003) and lower platelet counts (205 versus 293, P = 0.02). One CFLD patient had nodular regenerative hyperplasia. Longitudinally, mean platelet counts significantly declined in the CFLD group (from 310 to 230 U/L, P = 0.0005). Deceased CFLD patients had lower platelet counts than those alive with CFLD (143 versus 258 U/L, P = 0.004) or those deceased with no CFLD (143 versus 327U/L, P = 0.006).
Conclusion: Adult-onset CFLD may be more prevalent than previously described, which suggests a later wave of CFLD that impacts morbidity; routine liver tests, radiologic imaging, noninvasive fibrosis markers, and FibroScan can be used algorithmically to identify adult CFLD; and further evaluation in other CF cohorts should be performed for validation. (Hepatology 2017;66:591-601).
Published 2017. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
Figures



Comment in
-
Reply.Hepatology. 2018 Feb;67(2):799-800. doi: 10.1002/hep.29635. Epub 2018 Jan 1. Hepatology. 2018. PMID: 29105100 Free PMC article. No abstract available.
-
Cystic fibrosis liver disease in adults: Limits of noninvasive tests of fibrosis.Hepatology. 2018 Feb;67(2):798-799. doi: 10.1002/hep.29637. Epub 2018 Jan 1. Hepatology. 2018. PMID: 29105109 No abstract available.
References
-
- Colombo C. Liver disease in cystic fibrosis. Curr Opin Pulm Med. 2007;13:529–36. - PubMed
-
- Rowe SM, Miller S, Sorscher EJ. Mechanisms of disease: Cystic fibrosis. New England Journal of Medicine. 2005;352:1992–2001. - PubMed
-
- Cystic Fibrosis Foundation. Patient Registry Annual Data Report. 2011
-
- Bhardwaj S, Canlas K, Kahi C, et al. Hepatobiliary Abnormalities and Disease in Cystic Fibrosis Epidemiology and Outcomes Through Adulthood. Journal of Clinical Gastroenterology. 2009;43:858–864. - PubMed
-
- Sokol RJ, Durie PR. Recommendations for management of liver and biliary tract disease in cystic fibrosis. Cystic Fibrosis Foundation Hepatobiliary Disease Consensus Group. J Pediatr Gastroenterol Nutr. 1999;28(Suppl 1):S1–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
