

Pentraxin-3 modulates lipopolysaccharide-induced inflammatory response and attenuates liver injury
- PMID: 28422322
- PMCID: PMC5570620
- DOI: 10.1002/hep.29215
Pentraxin-3 modulates lipopolysaccharide-induced inflammatory response and attenuates liver injury
Abstract
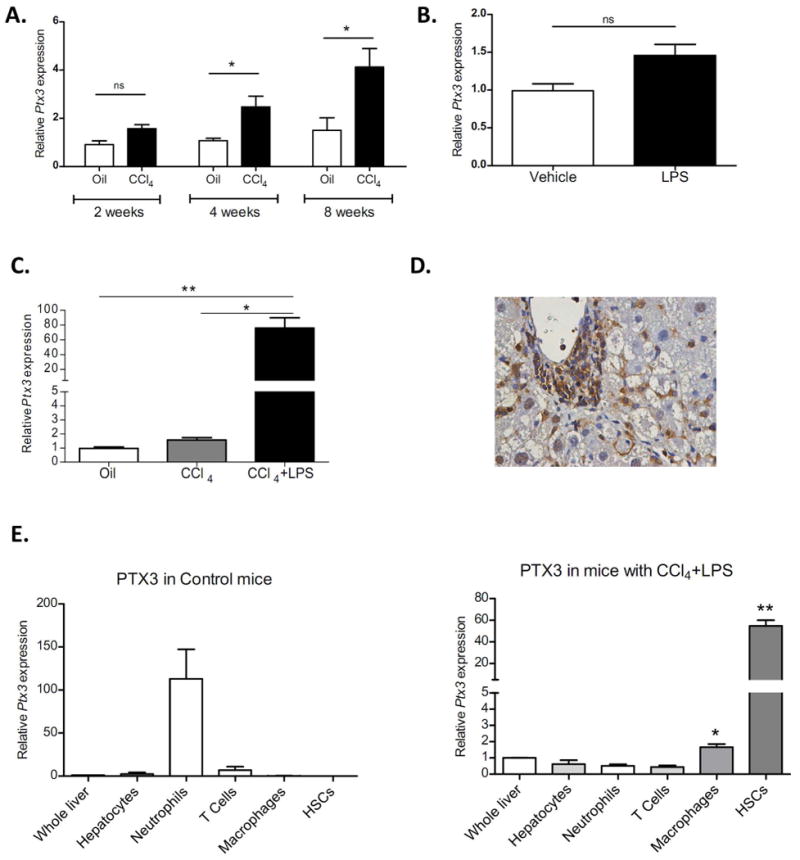
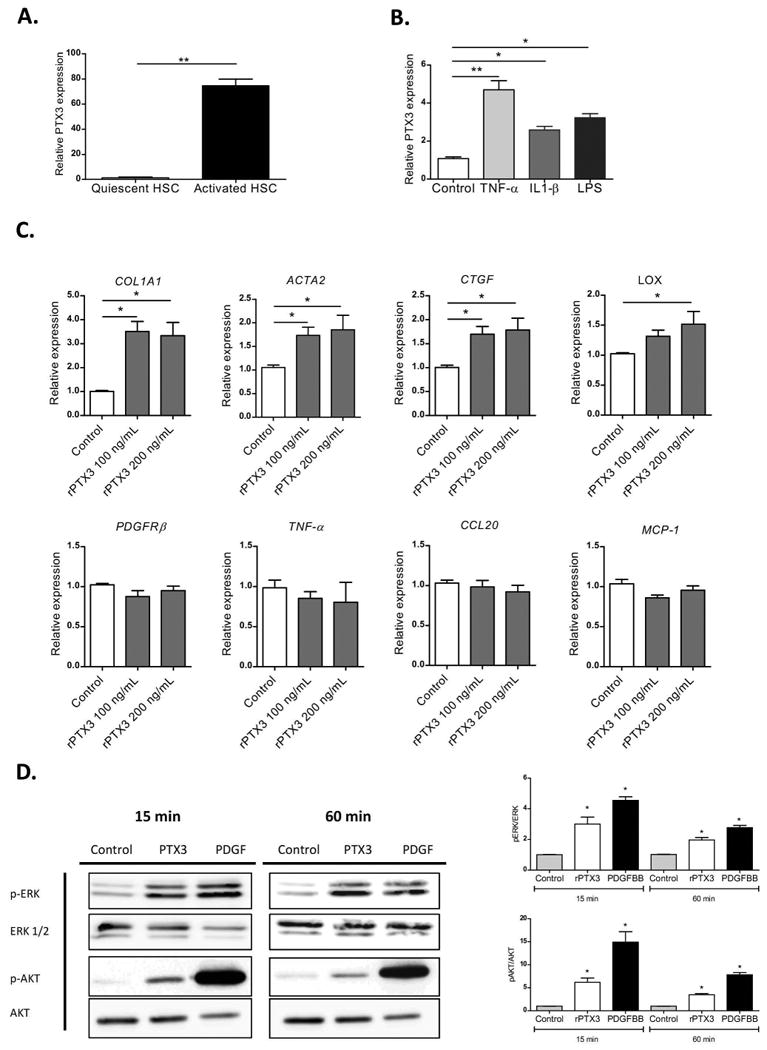
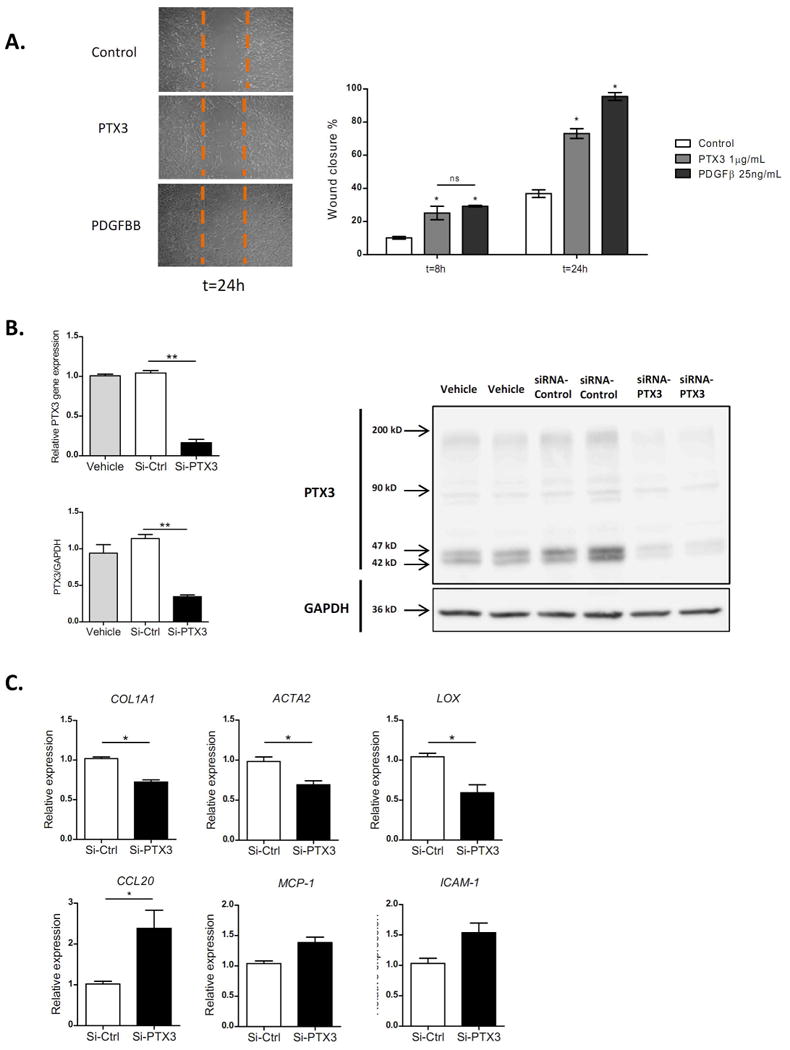
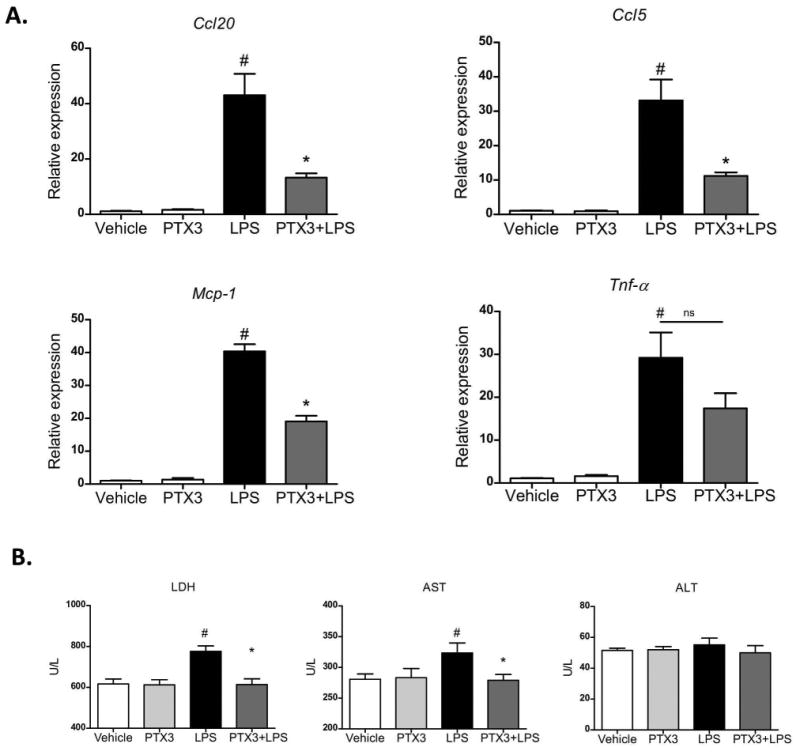
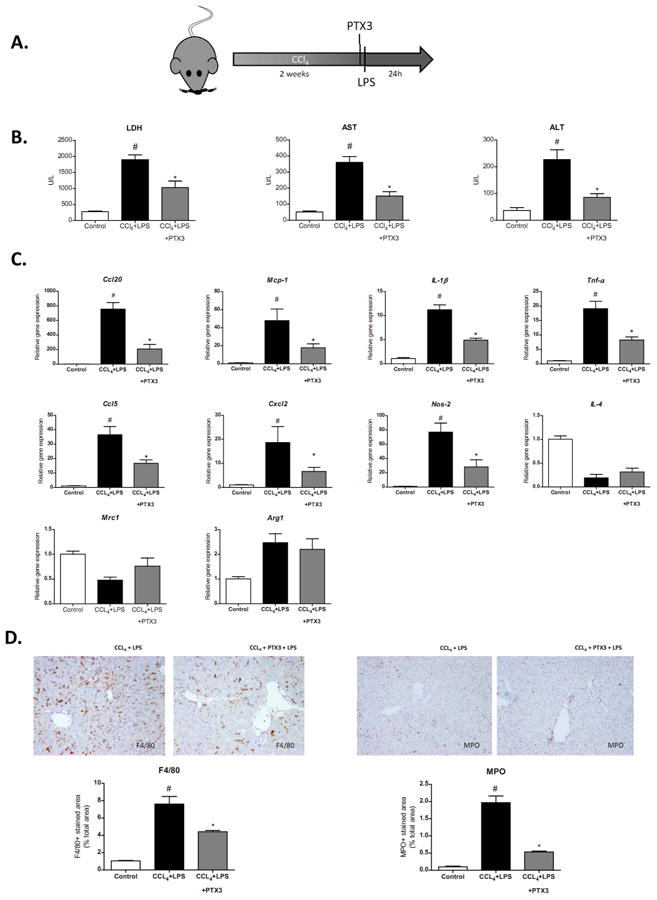
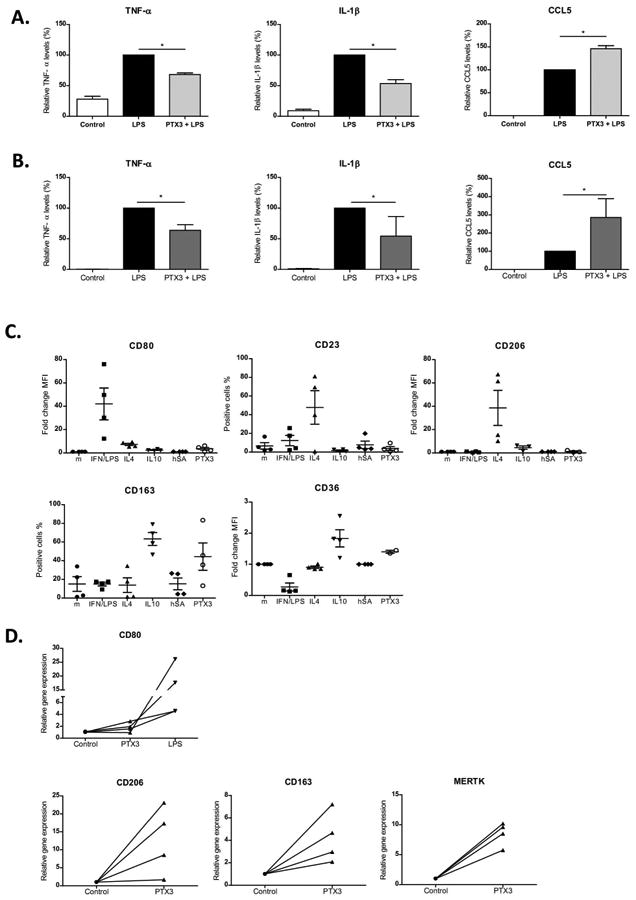
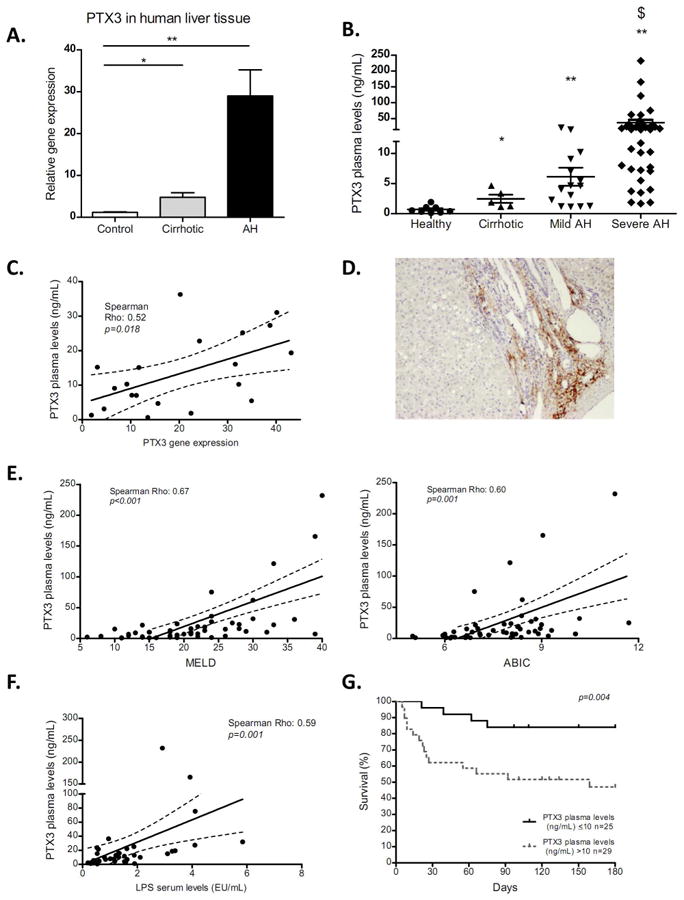
Acute-on-chronic liver injury is characterized by an important inflammatory response frequently associated with endotoxemia. In this context, acute-phase proteins such as Pentraxin-3 (PTX3) are released; however, little is known about their role in chronic liver disease. The aim of this study was to elucidate the role of PTX3 in liver injury. The role of PTX3 was evaluated in cultured human cells, liver tissue slices, and mice with acute-on-chronic liver injury. PTX3 expression was assessed in tissue and serum samples from 54 patients with alcoholic hepatitis. PTX3 expression was up-regulated in animal models of liver injury and strongly induced by lipopolysaccharide (LPS). Liver cell fractionation showed that macrophages and activated hepatic stellate cells were the main cell types expressing PTX3 in liver injury. Ex vivo and in vivo studies showed that PTX3 treatment attenuated LPS-induced liver injury, inflammation, and cell recruitment. Mechanistically, PTX3 mediated the hepatic stellate cell wound-healing response. Moreover, PTX3 modulated LPS-induced inflammation in human primary liver macrophages and peripheral monocytes by enhancing a TIR domain-containing adapter-inducing interferon-dependent response and favoring a macrophage interleukin-10-like phenotype. Additionally, hepatic and plasma PTX3 levels were increased in patients with alcoholic hepatitis, a prototypic acute-on-chronic condition; and its expression correlated with disease severity scores, endotoxemia, infections, and short-term mortality, thus suggesting that expression of PTX3 found in patients could be a counterregulatory response to injury.
Conclusion: Experimental and human evidence suggests that, in addition to being a potential biomarker for alcoholic hepatitis, PTX3 participates in the wound-healing response and attenuates LPS-induced liver injury and inflammation; therefore, administration of PTX3 could be a promising therapeutic strategy in acute-on-chronic conditions, particularly those associated with endotoxemia. (Hepatology 2017;66:953-968).
© 2017 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Figures
References
-
- Fujimoto M, Uemura M, Nakatani Y, Tsujita S, Hoppo K, Tamagawa T, et al. Plasma endotoxin and serum cytokine levels in patients with alcoholic hepatitis: relation to severity of liver disturbance. Alcohol Clin Exp Res [Internet] 2000;24:48S–54S. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10803780. - PubMed
-
- Arvaniti V, D'Amico G, Fede G, Manousou P, Tsochatzis E, Pleguezuelo M, et al. Infections in patients with cirrhosis increase mortality four-fold and should be used in determining prognosis. Gastroenterology [Internet] 2010;139:1246–1256.e5. Available from: http://dx.doi.org/10.1053/j.gastro.2010.06.019. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
