

Intraoperative centration during small incision lenticule extraction (SMILE)
- PMID: 28422822
- PMCID: PMC5406038
- DOI: 10.1097/MD.0000000000006076
Intraoperative centration during small incision lenticule extraction (SMILE)
Abstract
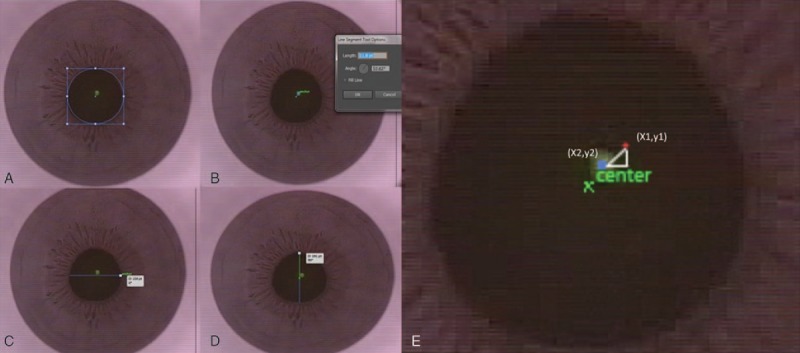
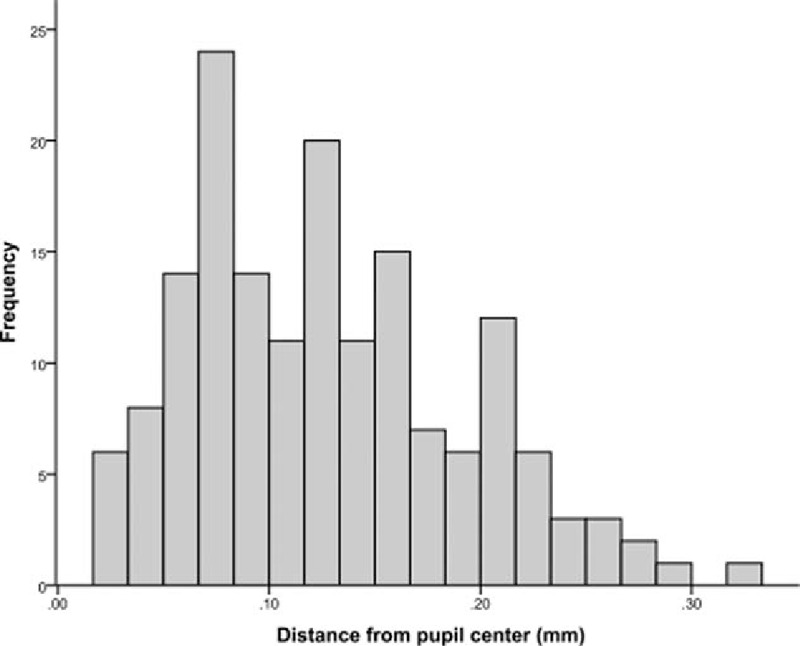
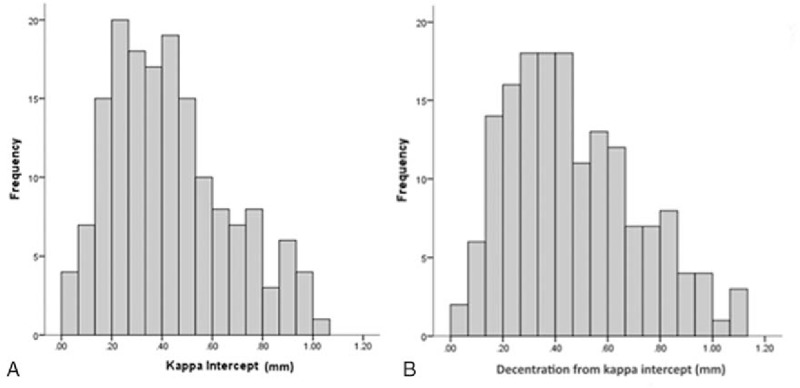
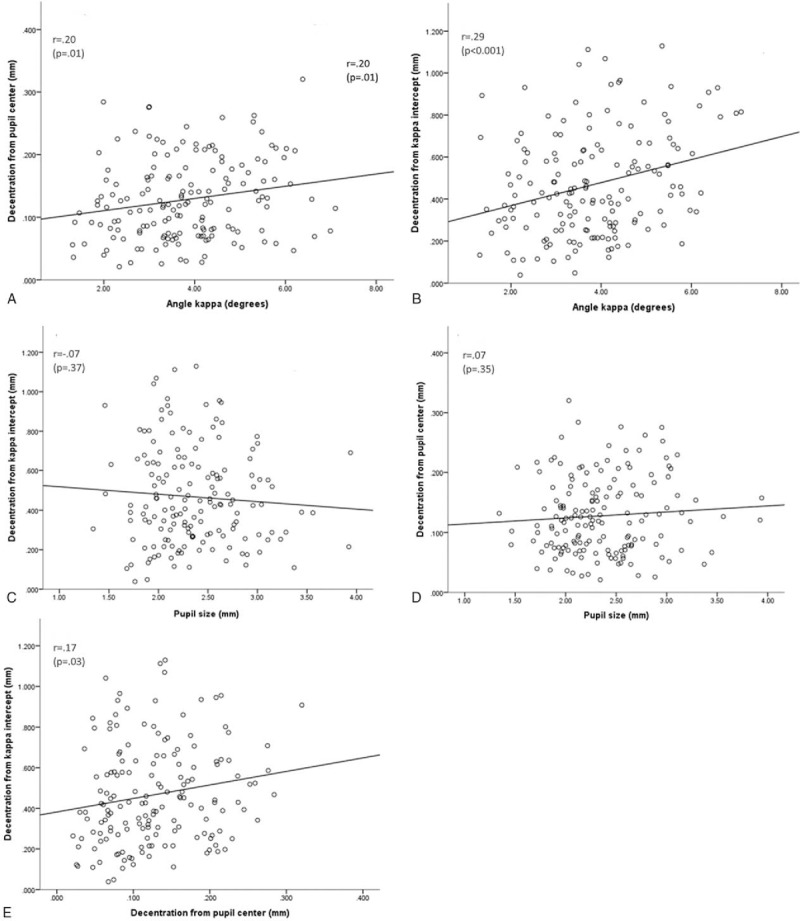
To evaluate intraoperative decentration from pupil center and kappa intercept during small incision lenticule extraction (SMILE) and its impact on visual outcomes.This was a retrospective noncomparative case series. A total of 164 eyes that underwent SMILE at the Singapore National Eye Center were included. Screen captures of intraoperative videos were analyzed. Preoperative and 3 month postoperative vision and refractive data were analyzed against decentration.The mean preoperative spherical equivalent (SE) was -5.84 ± 1.77. The mean decentration from the pupil center and from kappa intercept were 0.13 ± 0.06 mm and 0.47mm ± 0.25 mm, respectively. For efficacy and predictability, 69.6% and 95.0% of eyes achieved a visual acuity (VA) of 20/20 and 20/30, respectively, while 83.8% and 97.2% of eyes were within ±0.5D and ±1.0D of the targeted SE. When analyzed across 3 groups of decentration from the pupil center (<0.1 mm, 0.1-0.2 mm, and >0.2 mm), there was no statistically significant association between decentration, safety, efficacy, and predictability. When analyzed across 4 groups of decentration from kappa intercept (<0.2 mm, 0.2-<0.4 mm, 0.4-<0.6 mm, and ≥0.6 mm), there was a trend toward higher efficacy for eyes with decentration of kappa intercept between 0.4 and <0.6 mm (P = .097). A total of 85.4% of eyes in the 0.4 to <0.6 mm group had unaided distance VA of 20/20 or better, as compared to only 57.8% of eyes in ≥0.6 mm group.Decentration of 0.13 mm from the pupil center does not result in compromised visual outcomes. Decentration of greater than 0.6 mm from the kappa intercept may result in compromised visual outcomes. There was a trend toward better efficacy in eyes which had decentered treatment from 0.4 to <0.6 mm from the kappa intercept. Patients with a large kappa intercept (>0.6 mm) should have their lenticule created 0.4 to 0.6 mm from the kappa intercept and not close to the pupil.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Comparison of the Distribution of Lenticule Decentration Following SMILE by Pupil Center or Tear Film Mark Centration.J Refract Surg. 2020 Apr 1;36(4):239-246. doi: 10.3928/1081597X-20200310-01. J Refract Surg. 2020. PMID: 32267954
-
Relationship Between Decentration and Induced Corneal Higher-Order Aberrations Following Small-Incision Lenticule Extraction Procedure.Invest Ophthalmol Vis Sci. 2018 May 1;59(6):2316-2324. doi: 10.1167/iovs.17-23451. Invest Ophthalmol Vis Sci. 2018. PMID: 29847636
-
Mild decentration measured by a Scheimpflug camera and its impact on visual quality following SMILE in the early learning curve.Invest Ophthalmol Vis Sci. 2014 May 20;55(6):3886-92. doi: 10.1167/iovs.13-13714. Invest Ophthalmol Vis Sci. 2014. PMID: 24845636
-
Measurement of angle kappa and centration in refractive surgery.Curr Opin Ophthalmol. 2012 Jul;23(4):269-75. doi: 10.1097/ICU.0b013e3283543c41. Curr Opin Ophthalmol. 2012. PMID: 22569467 Review.
-
Angle Kappa and its importance in refractive surgery.Oman J Ophthalmol. 2013 Sep;6(3):151-8. doi: 10.4103/0974-620X.122268. Oman J Ophthalmol. 2013. PMID: 24379548 Free PMC article. Review.
Cited by
-
Will SMILE Become the New Benchmark of Corneal Laser Refractive Surgery?Asia Pac J Ophthalmol (Phila). 2019 Sep-Oct;8(5):351-354. doi: 10.1097/01.APO.0000579956.14784.91. Asia Pac J Ophthalmol (Phila). 2019. PMID: 31567435 Free PMC article. No abstract available.
-
Higher-order aberrations and visual quality after incision lenticule extraction surgery with intraoperative angle kappa adjustments between small and large kappa patients: A 2-year follow-up.Indian J Ophthalmol. 2023 May;71(5):1849-1854. doi: 10.4103/IJO.IJO_3017_22. Indian J Ophthalmol. 2023. PMID: 37203043 Free PMC article.
-
Astigmatism Correction Using SMILE.Asia Pac J Ophthalmol (Phila). 2019 Sep-Oct;8(5):391-396. doi: 10.1097/01.APO.0000580140.74826.f5. Asia Pac J Ophthalmol (Phila). 2019. PMID: 31490198 Free PMC article. Review.
-
Matched comparison of corneal higher order aberrations induced by SMILE to femtosecond assisted LASIK and to PRK in correcting moderate and high myopia: 3.00mm vs. 6.00mm.BMC Ophthalmol. 2021 May 15;21(1):216. doi: 10.1186/s12886-021-01987-3. BMC Ophthalmol. 2021. PMID: 33992084 Free PMC article.
-
Relationship of Location Between Tear Film Center and Corneal Vertex Following Small-Incision Lenticule Extraction.Ophthalmol Ther. 2022 Jun;11(3):1163-1174. doi: 10.1007/s40123-022-00496-w. Epub 2022 Apr 4. Ophthalmol Ther. 2022. PMID: 35378687 Free PMC article.
References
-
- Sugar A, Rapuano CJ, Culbertson WW, et al. Laser in situ keratomileusis for myopia and astigmatism: safety and efficacy; a report by the American Academy of Ophthalmology (Ophthalmic Technology Assessment). Ophthalmology 2002;109:175–87. - PubMed
-
- Sugar A. Ultrafast (femtosecond) laser refractive surgery. Curr Opin Ophthalmol 2002;13:246–9. - PubMed
-
- Shah R, Shah S, Sengupta S. Results of small incision lenticule extraction: all-in-one femtosecond laser refractive surgery. J Cataract Refract Surg 2011;37:127–37. - PubMed
-
- Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol 2011;95:335–9. - PubMed
-
- Reinstein DZ, Archer TJ, Randleman JB. Mathematical model tocompare the relative tensile strength of the cornea after PRK, LASIK, and small incision lenticule extraction. J Refract Surg 2013;29:454–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
