

Feasibility and safety of emergency laparoscopic partial splenectomy: A retrospective analysis
- PMID: 28422834
- PMCID: PMC5406050
- DOI: 10.1097/MD.0000000000006450
Feasibility and safety of emergency laparoscopic partial splenectomy: A retrospective analysis
Abstract
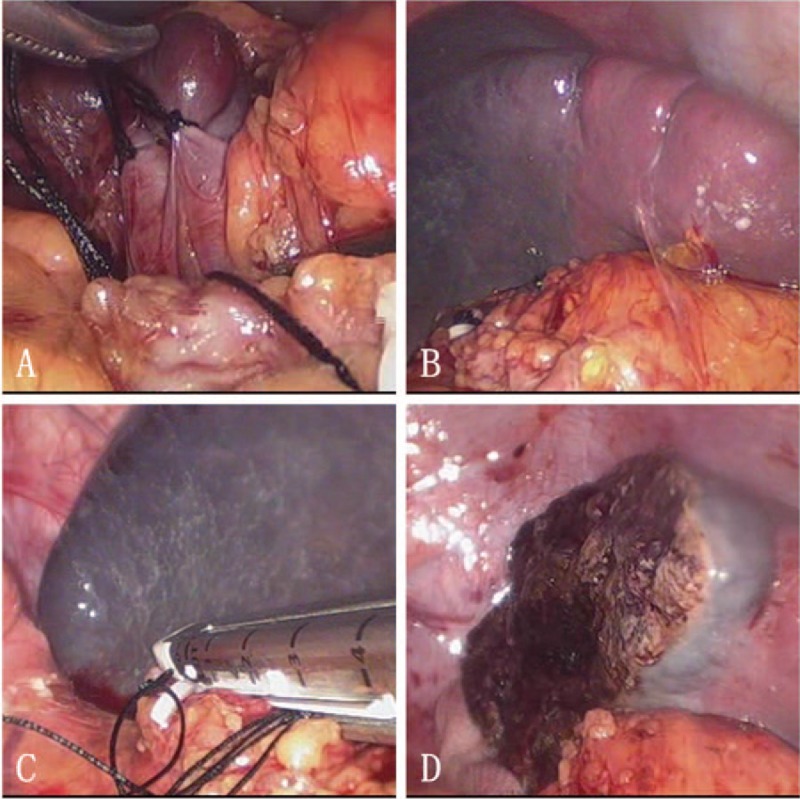
The increased awareness of asplenia-related life-threatening complications has led to the development of parenchyma sparing splenic resections in past few years. The aim of this study is to retrospectively analyze the feasibility and safety of laparoscopic partial splenectomy (LPS) in selected emergency patients.From January 2013 to December 2015, there were 46 emergency patients, diagnosed with splenic rupture, admitted in our department. Selection criteria for LPS: (1) Preoperative CT scan revealed single pole rupture without spleen pedicle injury; (2) BP>90/60 mm Hg and heart rates <120 bpm; (3) No sigh of multiple organ injury. Eventually, LPS was performed in 21 patients (Group LPS), while laparoscopic splenectomy (LS) was performed in 20 patients (Group LS).The main cause of splenic rupture was traffic accident, followed by blunt injury and high falling injury. Abdominal CT scan showed the mean longitudinal diameter of spleen of group LPS was 14.2 ± 1.8 cm (range 12-17 cm), while the size of remnant spleen was 5.5 ± 1.2 cm. Between 2 groups, operation time (LPS: 122.6 ± 17.2 min vs LS: 110.5 ± 18.7 minutes, P = .117), and intraoperative blood loss (LPS: 174 ± 22 mL vs LS: 169 ± 29 mL, P = .331) were similar. There were 2 patients suffered subsequent unstable vital sign altering during mobilization when performing LPS. Conversion to LS (2/21, 9.52%) was decided and successfully completed. Although there was no patient suffered postoperative OPSI or thrombocytosis events in both groups after 6-month follow-up, the mean platelets and leukocyte count were significantly lower in group LPS. Splenic regrowth was evaluated in 20 patients of group LPS. And the mean regrowth of splenic volume reached 19% (10%-26%).Due to its minimal invasive effect and functional splenic tissue preservation, LPS may be a safe and feasible approach for emergency patients. And prospective trials with clear inclusion criteria are needed to proof the benefit of LPS.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Emergency laparoscopic partial splenectomy for ruptured spleen: a case report.World J Gastroenterol. 2014 Dec 14;20(46):17670-3. doi: 10.3748/wjg.v20.i46.17670. World J Gastroenterol. 2014. PMID: 25516684 Free PMC article.
-
Laparoscopic radiofrequency ablation for traumatic splenic rupture.J Surg Res. 2013 Dec;185(2):711-6. doi: 10.1016/j.jss.2013.06.018. Epub 2013 Jul 1. J Surg Res. 2013. PMID: 23859132 Clinical Trial.
-
Laparoscopic splenectomy for splenic littoral cell angioma.World J Gastroenterol. 2015 Jun 7;21(21):6660-4. doi: 10.3748/wjg.v21.i21.6660. World J Gastroenterol. 2015. PMID: 26074704 Free PMC article.
-
Emergency transumbilical single-incision laparoscopic splenectomy for the treatment of traumatic rupture of the spleen: report of the first case and literature review.Surg Innov. 2011 Jun;18(2):185-8. doi: 10.1177/1553350611403767. Epub 2011 Apr 25. Surg Innov. 2011. PMID: 21521700 Review.
-
Comparative treatment and literature review for laparoscopic splenectomy alone versus preoperative splenic artery embolization splenectomy.Surg Endosc. 2012 Oct;26(10):2758-66. doi: 10.1007/s00464-012-2270-z. Epub 2012 May 12. Surg Endosc. 2012. PMID: 22580870 Review.
Cited by
-
Laparoscopic splenectomy after trauma: Who, when and how. A systematic review.J Minim Access Surg. 2021 Apr-Jun;17(2):141-146. doi: 10.4103/jmas.JMAS_149_19. J Minim Access Surg. 2021. PMID: 31670290 Free PMC article. Review.
-
Comparison of perioperative outcomes between laparoscopic and open partial splenectomy in children and adolescents.World J Gastrointest Surg. 2021 Sep 27;13(9):979-987. doi: 10.4240/wjgs.v13.i9.979. World J Gastrointest Surg. 2021. PMID: 34621474 Free PMC article.
-
Partial splenectomy: A case series and systematic review of the literature.Ann Hepatobiliary Pancreat Surg. 2018 May;22(2):116-127. doi: 10.14701/ahbps.2018.22.2.116. Epub 2018 May 30. Ann Hepatobiliary Pancreat Surg. 2018. PMID: 29896572 Free PMC article.
-
The safety and feasibility of laparoscopic partial splenectomy: analysis of perioperative indications from different vascular subtypes and improvement of surgical approach.Surg Endosc. 2024 Dec;38(12):7329-7340. doi: 10.1007/s00464-024-11270-3. Epub 2024 Oct 21. Surg Endosc. 2024. PMID: 39433590 Free PMC article.
-
Laparoscopic surgery for splenic injuries in the era of non-operative management: current status and future perspectives.Surg Today. 2021 Jul;51(7):1075-1084. doi: 10.1007/s00595-020-02177-2. Epub 2020 Nov 16. Surg Today. 2021. PMID: 33196920 Free PMC article. Review.
References
-
- Lynch AM, Kapila R. Overwhelming postsplenectomy infection. Infect Dis Clin North Am 1996;10:693–707. PubMed PMID: 8958164. - PubMed
-
- Robinette CD, Fraumeni JF., Jr Splenectomy and subsequent mortality in veterans of the 1939–45 war. Lancet 1977;2:127–9. PubMed PMID: 69206. - PubMed
-
- Schilling RF. Spherocytosis, splenectomy, strokes, and heat attacks. Lancet 1997;350:1677–8. PubMed PMID: 9400518. - PubMed
-
- Holdsworth RJ, Irving AD, Cuschieri A. Postsplenectomy sepsis and its mortality rate: actual versus perceived risks. Brit J Surg 1991;78:1031–8. PubMed PMID: 1933181. - PubMed
-
- Di Sabatino A, Carsetti R, Corazza GR. Post-splenectomy and hyposplenic states. Lancet 2011;378:86–97. PubMed PMID: 21474172. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
