

Case report: A female case of isolated IgG4-related sclerosing cholangitis mimicking cholangiocarcinoma
- PMID: 28422840
- PMCID: PMC5406056
- DOI: 10.1097/MD.0000000000006542
Case report: A female case of isolated IgG4-related sclerosing cholangitis mimicking cholangiocarcinoma
Abstract
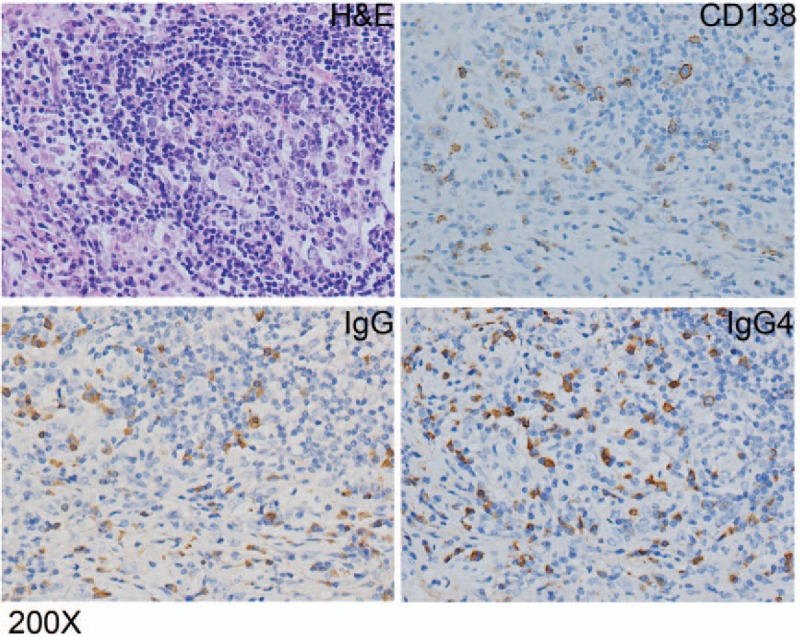
Rationale: IgG4-related disease is a newly recognized fibroinflammatory disorder, characterized by tumefactive lesions, storiform fibrosis and IgG4-positive plasma cells infiltration. IgG4-related sclerosing cholangitis (IgG4-SC) is the most common extrapancreatic manifestation of IgG4-related disease, but it is frequently associated with autoimmune pancreatitis(AIP). Only few case was reported to be diagnosed with IgG4-SC in the absence of AIP, with a striking male preponderance. Here we report a female case of isolated IgG4 related sclerosing cholangitis mimicking cholangiocarcinoma.
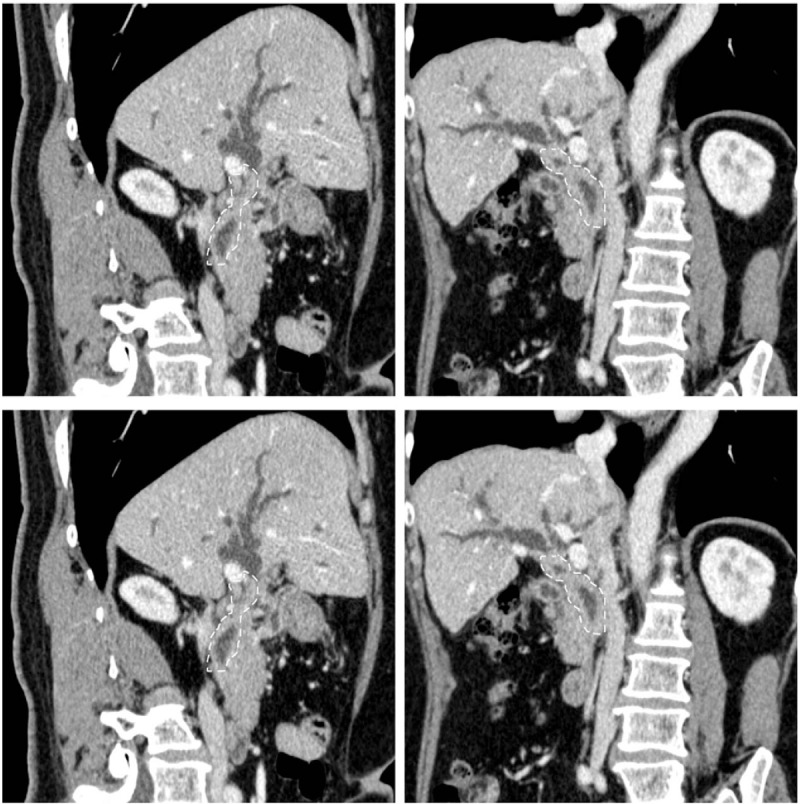
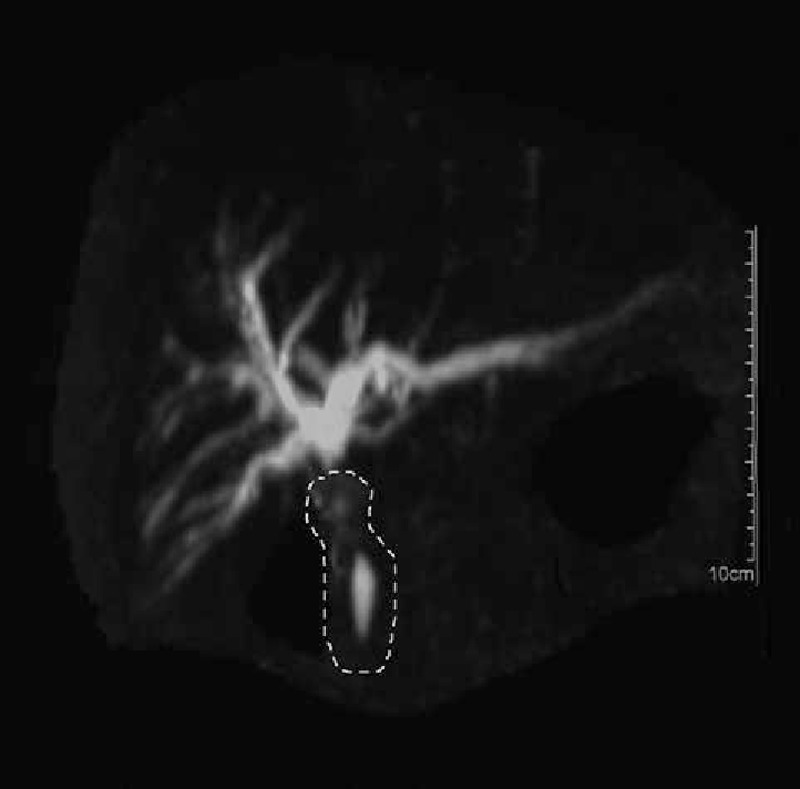
Patient concerns: A 58-year-old woman complaint of one-month history of jaundice and right upper quadrant discomfort, and the biliary reconstruction showed full-length wall thickening and segmental stenosis.
Diagnoses: Cholangiocarcinoma was then diagnosed.
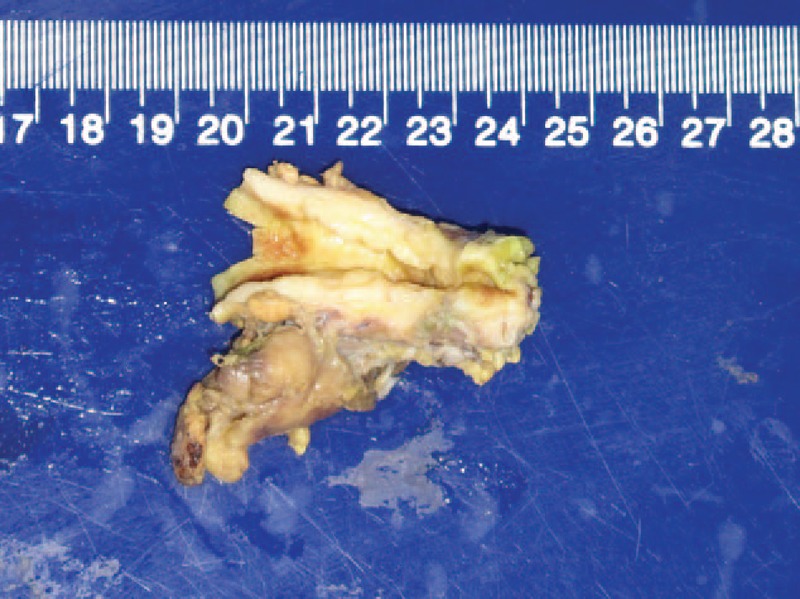
Interventions: Choledochoplasty was performed, followed by Roux-en-Y anastomosis.
Outcomes: However, pathological examination revealed IgG4-related sclerosing cholangitis (IgG4-SC) and the retrospective measurement of serum IgG4 was 346 mg/dL post-operatively. The patient was followed for another nine monthswithout recurrence.
Lessons: The differential diagnosis between cholangiocarcinoma and IgG4-SC is challenging due to significant overlap of clinical manifestations, lab tests and imaging characteristics. However, as an afterthought of this case, typical cholangiocarcinoma rarely presents full-length wall thickening. What the case taught us was pre-operative IgG4 measurement for patients with long bile duct involvement was highly recommended in order to rule out IgG4-SC.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
IgG4-related sclerosing cholangitis in the absence of autoimmune pancreatitis mimicking extrahepatic cholangiocarcinoma.Scand J Gastroenterol. 2015 Apr;50(4):447-53. doi: 10.3109/00365521.2014.962603. Epub 2015 Jan 30. Scand J Gastroenterol. 2015. PMID: 25635498
-
IgG4-related Sclerosing Cholangitis Mimicking Cholangiocarcinoma Diagnosed by Endoscopic Ultrasound-guided Fine-needle Aspiration.Intern Med. 2020 Apr 1;59(7):945-950. doi: 10.2169/internalmedicine.3905-19. Epub 2019 Dec 26. Intern Med. 2020. PMID: 31875638 Free PMC article.
-
Clinical clues to suspicion of IgG4-associated sclerosing cholangitis disguised as primary sclerosing cholangitis or hilar cholangiocarcinoma.J Gastroenterol Hepatol. 2010 Dec;25(12):1831-7. doi: 10.1111/j.1440-1746.2010.06411.x. J Gastroenterol Hepatol. 2010. PMID: 21091993
-
Endoscopic retrograde cholangiopancreatography and intraductal ultrasonography in the diagnosis of autoimmune pancreatitis and IgG4-related sclerosing cholangitis.J Med Ultrason (2001). 2021 Oct;48(4):573-580. doi: 10.1007/s10396-021-01114-1. Epub 2021 Jul 31. J Med Ultrason (2001). 2021. PMID: 34331625 Review.
-
Biliary and hepatic involvement in IgG4-related disease.Aliment Pharmacol Ther. 2014 Dec;40(11-12):1251-61. doi: 10.1111/apt.12988. Epub 2014 Oct 13. Aliment Pharmacol Ther. 2014. PMID: 25312536 Review.
Cited by
-
Highlighting the importance of early diagnosis in progressive multi-organ involvement of IgG4-related disease: A case report and review of literature.World J Clin Cases. 2018 Nov 6;6(13):707-715. doi: 10.12998/wjcc.v6.i13.707. World J Clin Cases. 2018. PMID: 30430130 Free PMC article.
-
IgG4-related sclerosing cholangitis mimicking hilar cholangiocarcinoma (Klatskin tumor): a case report of a challenging disease and review of the literature.Innov Surg Sci. 2018 May 25;3(2):157-163. doi: 10.1515/iss-2018-0010. eCollection 2018 Jun. Innov Surg Sci. 2018. PMID: 31579779 Free PMC article.
-
IgG4-related sclerosing cholangitis, a mimicker of the cholangiocarcinoma: A case report.Clin Case Rep. 2023 Feb 8;11(2):e6935. doi: 10.1002/ccr3.6935. eCollection 2023 Feb. Clin Case Rep. 2023. PMID: 36789321 Free PMC article.
-
Isolated mass-forming IgG4-related sclerosing cholangitis masquerading as extrahepatic cholangiocarcinoma: A case report.World J Clin Cases. 2021 Oct 16;9(29):8773-8781. doi: 10.12998/wjcc.v9.i29.8773. World J Clin Cases. 2021. PMID: 34734055 Free PMC article.
-
Amputation neuroma derived from a remnant cystic duct 30 years after cholecystectomy: A case report.Int J Surg Case Rep. 2019;64:184-187. doi: 10.1016/j.ijscr.2019.10.011. Epub 2019 Oct 12. Int J Surg Case Rep. 2019. PMID: 31671354 Free PMC article.
References
-
- Stone J, Zen Y. IgG4-related disease. N Engl J Med 2012;366:539–51. - PubMed
-
- Lin J, Cummings OW, Greenson JK, et al. IgG4-related sclerosing cholangitis in the absence of autoimmune pancreatitis mimicking extrahepatic cholangiocarcinoma. Scand J Gastroenterol 2015;50:447–53. - PubMed
-
- Ghazale A, Chari ST, Zhang L, et al. Immunoglobulin G4-associated cholangitis: clinical profile and response to therapy. Gastroenterology 2008;134:706–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
