

Ultrasound is helpful to differentiate Bethesda class III thyroid nodules: A PRISMA-compliant systematic review and meta-analysis
- PMID: 28422844
- PMCID: PMC5406060
- DOI: 10.1097/MD.0000000000006564
Ultrasound is helpful to differentiate Bethesda class III thyroid nodules: A PRISMA-compliant systematic review and meta-analysis
Abstract
Background: Fine-needle aspiration (FNA) is the most dependable tool to triage thyroid nodules for medical or surgical management. However, Bethesda class III cytology, namely "follicular lesion of undetermined significance" (FLUS) or "atypia of undetermined significance" (AUS), is a major limitation of the US-FNA in assessing thyroid nodules. As the most important imaging method, ultrasound (US) has a high efficacy in diagnosing thyroid nodules. This meta-analysis aimed to assess the role of US in evaluating Bethesda class III thyroid nodules.
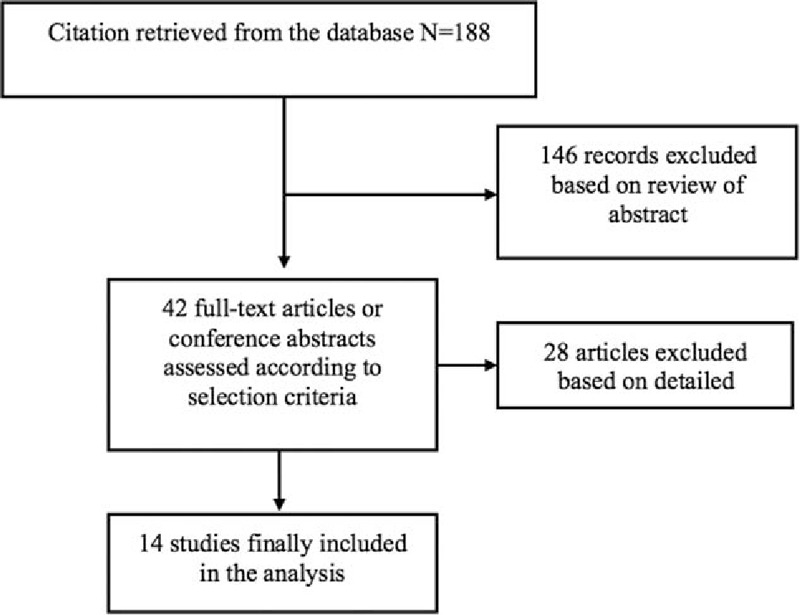
Methods: With keywords "Undetermined Significance," "Bethesda Category III," "Bethesda system," "Cytological Subcategory," "AUS/FLUS," "Atypia of Undetermined Significance," and "Ultrasound/US," papers in PubMed, Cochrane Library, Medline, Web of Science, Embase, and Google Scholar from inception to December 2016 were searched. A meta-analysis of these trials was then performed for evaluating the diagnostic value of thyroid ultrasound in Bethesda Category III thyroid nodules.
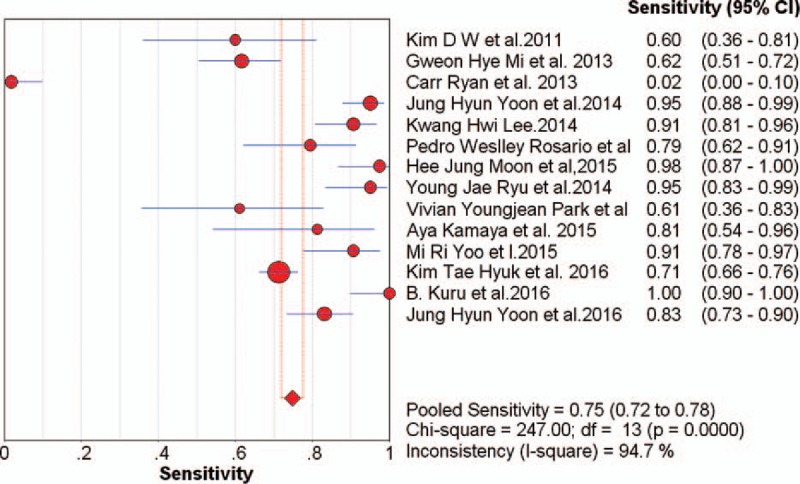
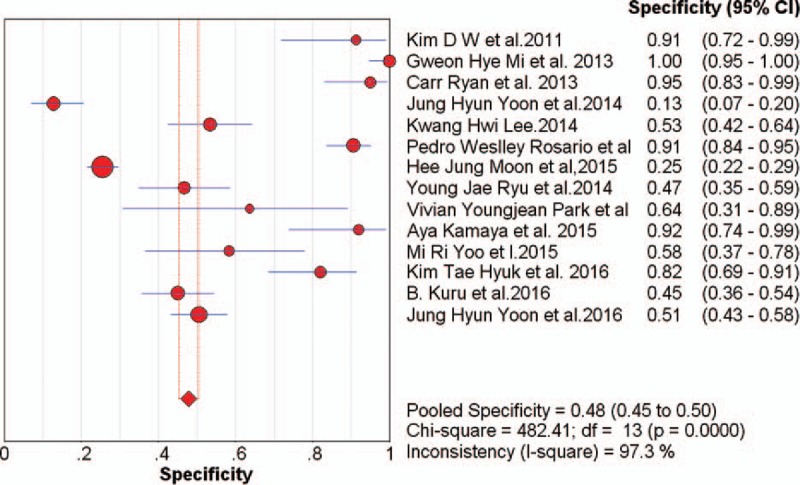
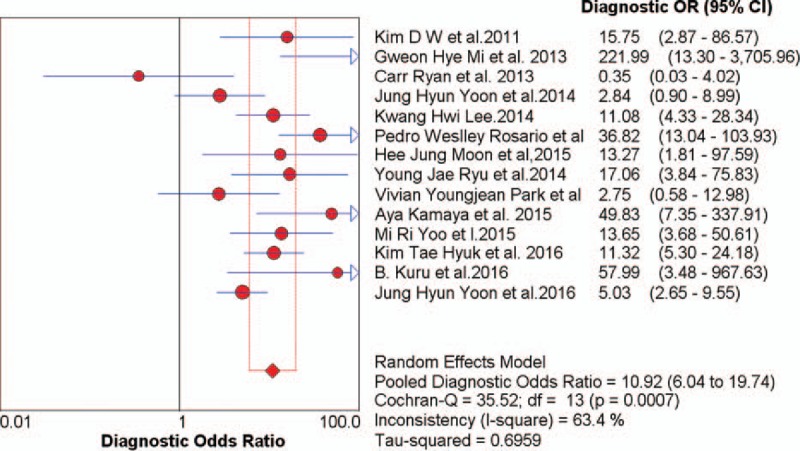
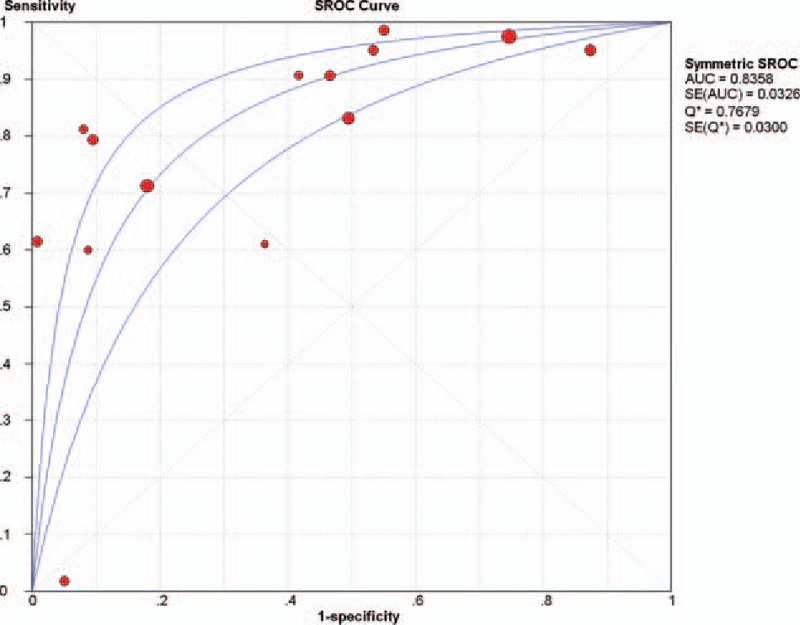
Results: Fourteen studies including 2405 nodules were analyzed. According to the criteria for US diagnosis of thyroid nodules in each article, with any one of suspicious features as indictors of malignancy, US had a pooled sensitivity of 0.75 (95% CI 0.72-0.78) and a pooled specificity of 0.48 (95% CI 0.45-0.50) in evaluating Bethesda Class III Nodules. The pooled diagnostic odds ratio was 10.92 (95% CI 6.04-19.74). The overall area under the curve was 0.84 and the Q* index was 0.77. With any 2 or 3 of US suspicious features as indictors of malignancy, the sensitivity and specificity were 0.77 (95% CI 0.71-0.83) and 0.54 (95% CI 0.51-0.58), 0.66 (95% CI 0.59-0.73) and 0.71 (95% CI 0.68-0.74), respectively.
Conclusions: US was helpful for differentiating benign and malignant Bethesda class III thyroid nodules, with the more suspicious features, the more likely to be malignant.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Diagnostic Performance of Ultrasound vs Ultrasound-Guided FNAC in Thyroid Nodules: Data From the ElaTION Trial.J Clin Endocrinol Metab. 2025 Jun 17;110(7):1997-2006. doi: 10.1210/clinem/dgae682. J Clin Endocrinol Metab. 2025. PMID: 39359050 Free PMC article. Clinical Trial.
-
The additive value of real-time elastography to thyroid ultrasound in detecting papillary carcinoma in nodules over 20 mm in diameter.Endocrine. 2025 Jul;89(1):177-185. doi: 10.1007/s12020-025-04248-1. Epub 2025 Apr 24. Endocrine. 2025. PMID: 40274686
-
Diagnostic accuracy of preoperative ultrasonography-guided fine-needle aspiration biopsy in distinguishing malignancy in large thyroid nodules: A systematic review, meta-analysis, and meta-regression.Narra J. 2025 Apr;5(1):e1120. doi: 10.52225/narra.v5i1.1120. Epub 2025 Feb 25. Narra J. 2025. PMID: 40352242 Free PMC article.
-
Qualitative elastography can replace thyroid nodule fine-needle aspiration in patients with soft thyroid nodules. A systematic review and meta-analysis.Eur J Radiol. 2015 Apr;84(4):652-61. doi: 10.1016/j.ejrad.2015.01.003. Epub 2015 Jan 16. Eur J Radiol. 2015. PMID: 25638577
-
Sonographic features of medullary thyroid carcinomas--a systematic review and meta-analysis.Endokrynol Pol. 2014;65(4):314-8. doi: 10.5603/EP.2014.0043. Endokrynol Pol. 2014. PMID: 25185855
Cited by
-
Machine Learning by Ultrasonography for Genetic Risk Stratification of Thyroid Nodules.JAMA Otolaryngol Head Neck Surg. 2020 Jan 1;146(1):36-41. doi: 10.1001/jamaoto.2019.3073. JAMA Otolaryngol Head Neck Surg. 2020. PMID: 31647509 Free PMC article.
-
Do ACR TI-RADS scores demonstrate unique thyroid molecular profiles?Ultrasonography. 2022 Jul;41(3):480-492. doi: 10.14366/usg.21130. Epub 2021 Dec 20. Ultrasonography. 2022. PMID: 35189676 Free PMC article.
-
ACR TI-RADS and ATA US scores are helpful for the management of thyroid nodules with indeterminate cytology.BMC Endocr Disord. 2019 Oct 29;19(1):112. doi: 10.1186/s12902-019-0429-5. BMC Endocr Disord. 2019. PMID: 31664992 Free PMC article.
-
Prediction of thyroid nodule histopathology by expert ultrasound evaluation.Endocr Connect. 2021 Jul 17;10(7):776-781. doi: 10.1530/EC-21-0192. Endocr Connect. 2021. PMID: 34156970 Free PMC article.
-
Prevalence of thyroid carcinoma in nodules with thy 3 cytology: the role of preoperative ultrasonography and strain elastography.Thyroid Res. 2021 Apr 9;14(1):7. doi: 10.1186/s13044-021-00098-x. Thyroid Res. 2021. PMID: 33836771 Free PMC article.
References
-
- Tan GH, Gharib H. Thyroid incidentalomas: management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Ann Intern Med 1997;126:226–31. - PubMed
-
- Guth S, Theune U, Aberle J, et al. Very high prevalence of thyroid nodules detected by high frequency (13 MHz) ultrasound examination. Eur J Clin Invest 2009;39:699–706. - PubMed
-
- Hegedüs L. Clinical practice. The thyroid nodule. N Engl J Med 2004;351:1764–71. - PubMed
-
- Mandel SJ. A 64-year-old woman with a thyroid nodule. JAMA 2004;292:2632–42. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
