

Prognosis of surgery combined with different adjuvant therapies in esophageal cancer treatment: a network meta-analysis
- PMID: 28423740
- PMCID: PMC5482659
- DOI: 10.18632/oncotarget.16193
Prognosis of surgery combined with different adjuvant therapies in esophageal cancer treatment: a network meta-analysis
Abstract
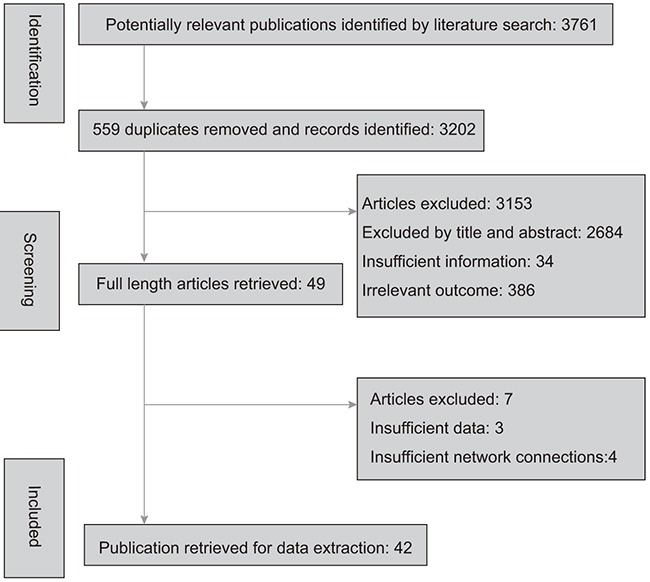
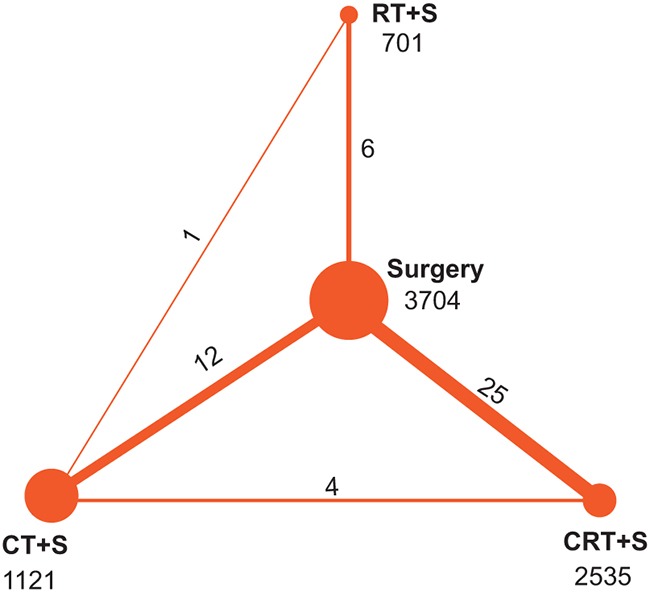
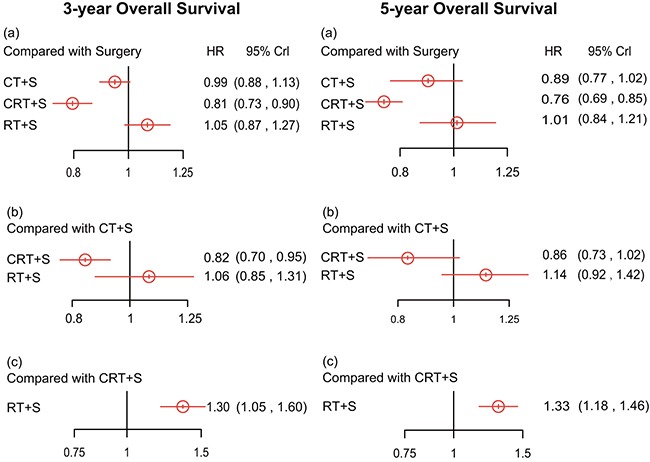
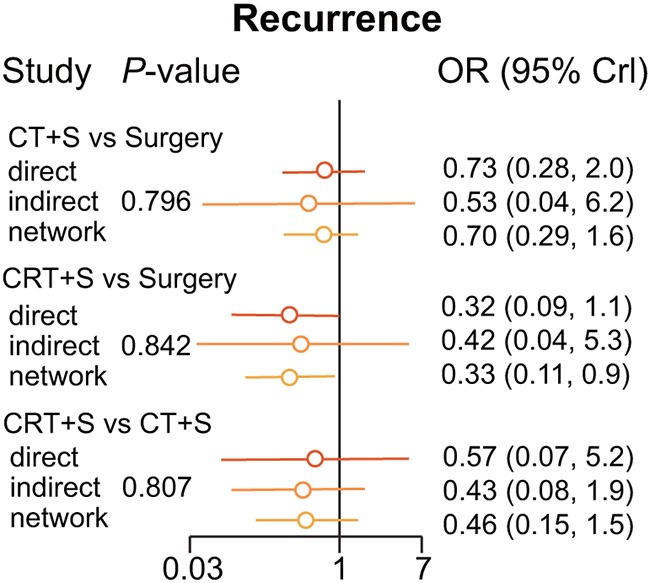
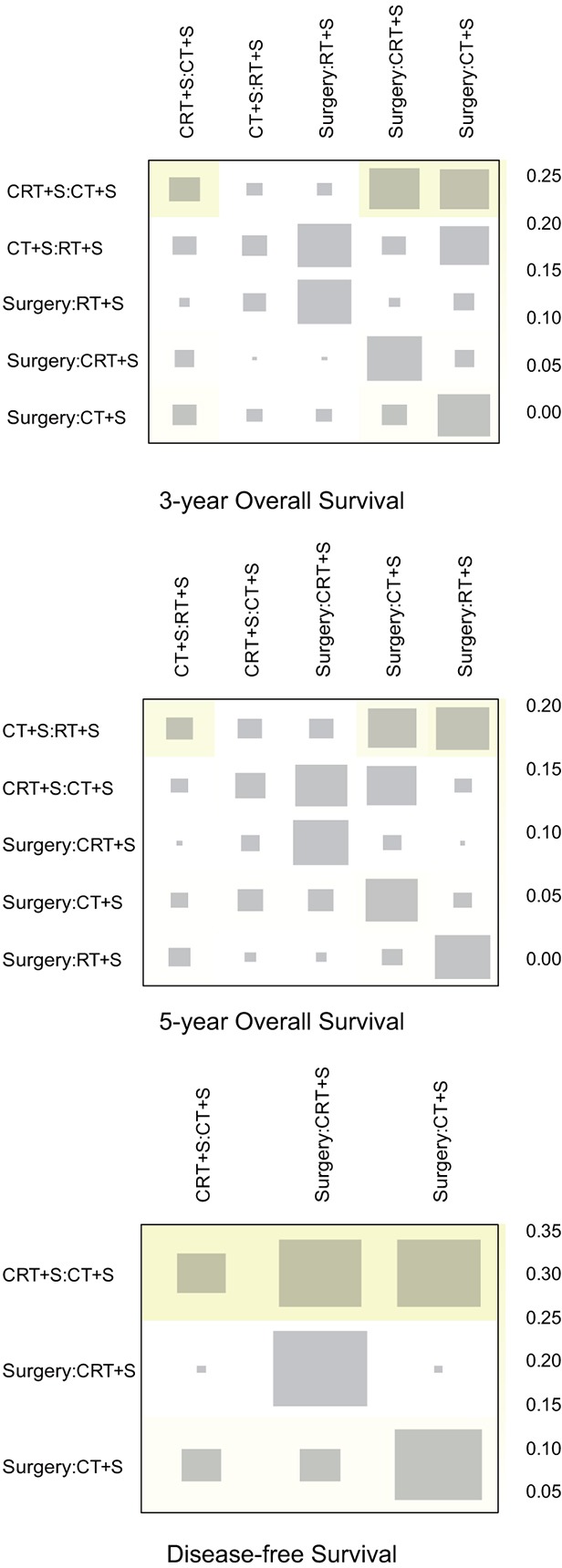
This network meta-analysis was conducted to assess whether the efficacy of surgery with adjuvant therapies, including radiotherapy (RT+S), chemotherapy (CT+S), and chemoradiotherapy (CRT+S) have better performance in esophageal cancer treatment and management. PubMed and EMBASE were used to search for relevant trials. Both conventional pair-wise and network meta-analyses were carried out. The surface under the cumulative ranking curve (SUCRA) was used to rank interventions based on the efficacy of the treatment method. As for 3-year overall survival (OS), CRT+S showed the highest efficacy (CRT+S vs.
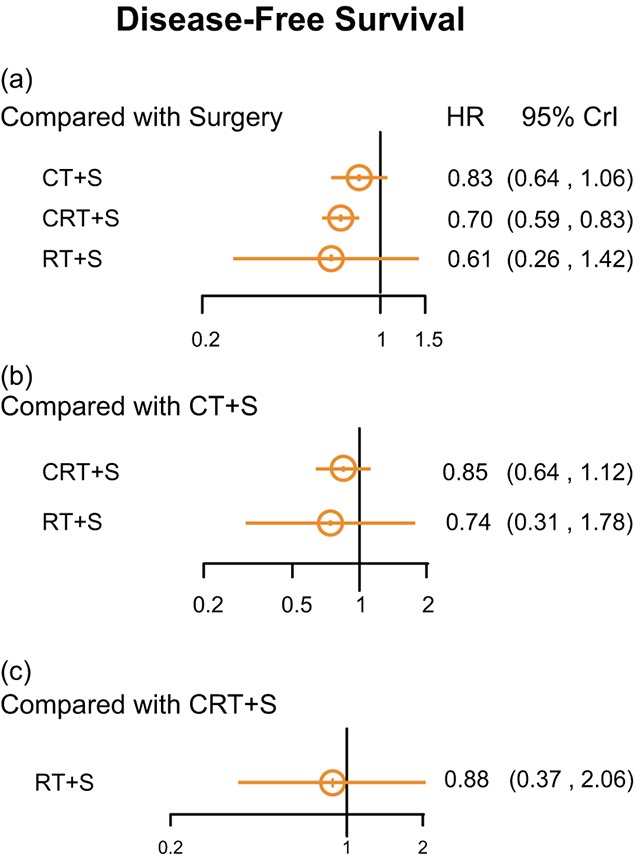
Surgery: HR=0.81, 95% CrI =0.73-0.90; CRT+S vs. CT+S: HR=0.82, 95% CrI =0.70-0.95; CRT+S vs. RT+S: HR=0.77, 95% CrI =0.62-0.95). For disease-free survival, CRT+S showed efficacy over CT+S ((HR =0.70, 95% CrI =0. 59-0.83). In conclusion, CRT+S showed a better performance for survival outcomes and ranks best among all therapies. The results of our study can provide guidance for medical decisions and treatment options that may help clinical practitioners improve the efficacy of EC treatment.
Keywords: adjuvant therapies; chemotherapy; esophageal cancer; radiotherapy; surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Esophageal cancer: epidemiology, pathogenesis and prevention. Nat Clin Pract Gastroenterol Hepatol. 2008;5:517–526. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. - PubMed
-
- Parkin DM, Muir CS, Cancer Incidence in Five Continents Comparability and quality of data. IARC Sci Publ. 1992:45–173. - PubMed
-
- Crew KD, Neugut AI. Epidemiology of upper gastrointestinal malignancies. Semin Oncol. 2004;31:450–464. - PubMed
-
- Bollschweiler E, Wolfgarten E, Gutschow C, Holscher AH. Demographic variations in the rising incidence of esophageal adenocarcinoma in white males. Cancer. 2001;92:549–555. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
