

Multiple myeloma of the spine
- PMID: 28423980
- PMCID: PMC5480803
- DOI: 10.1177/1971400917699426
Multiple myeloma of the spine
Abstract
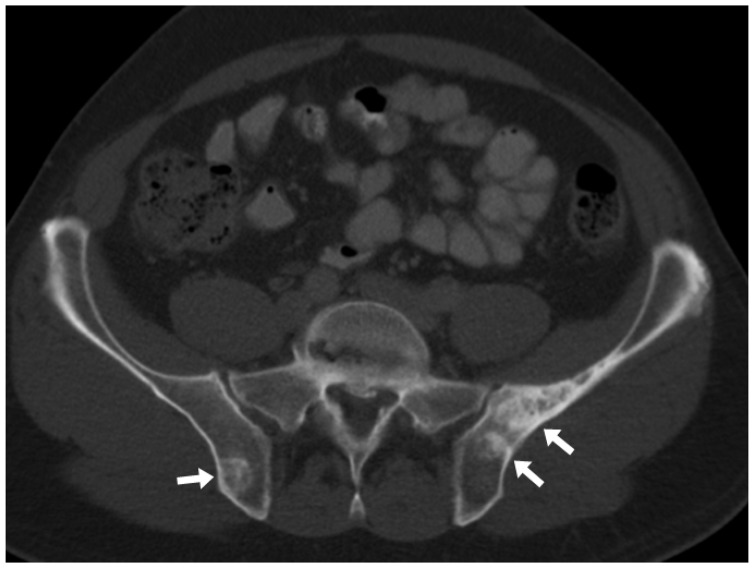
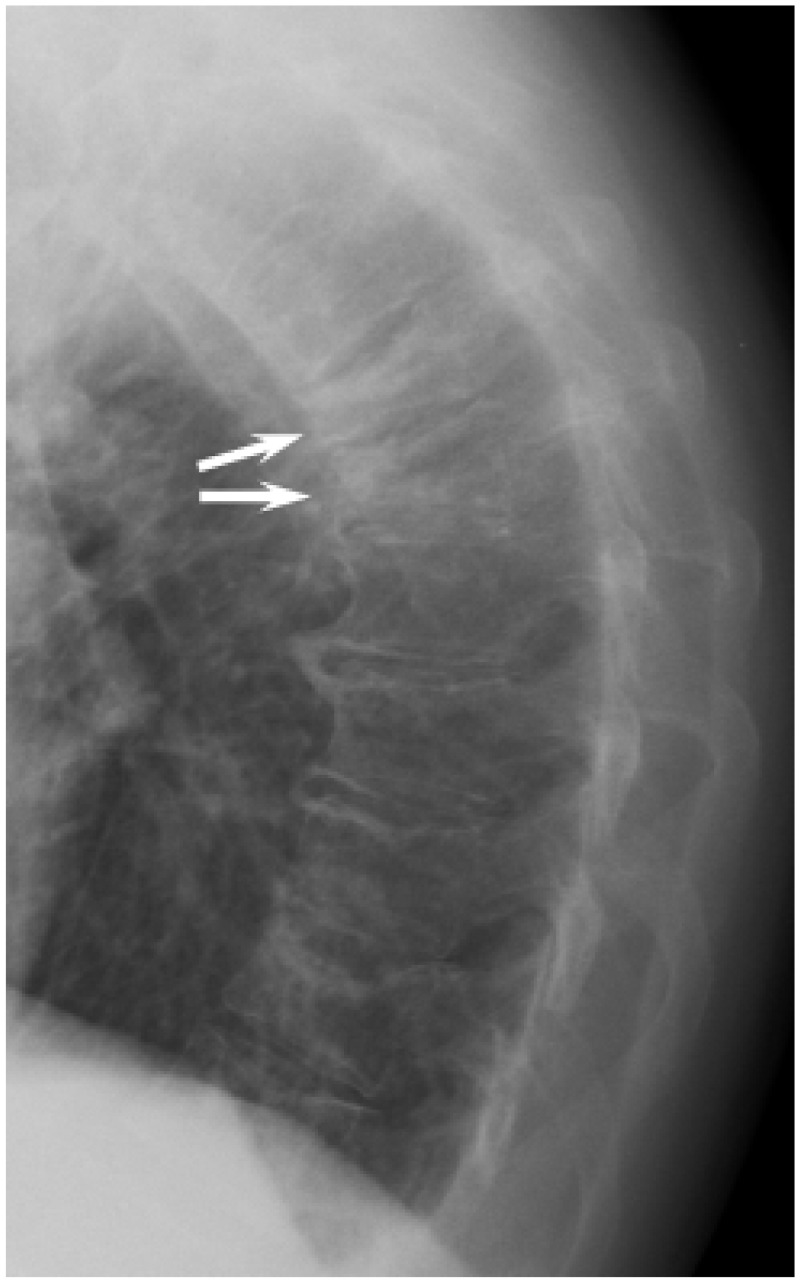
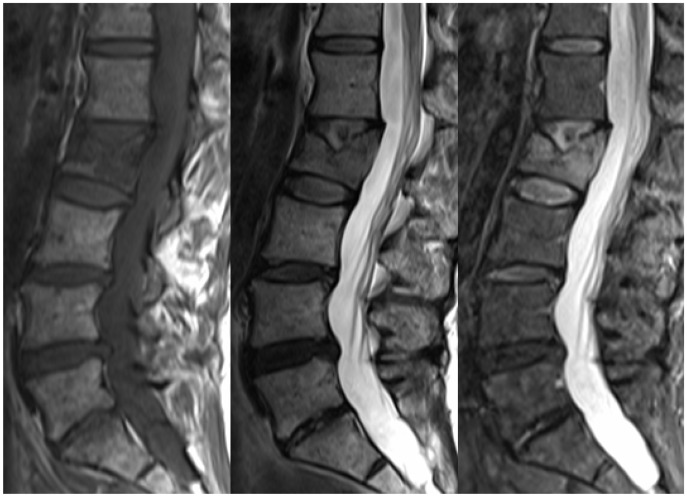
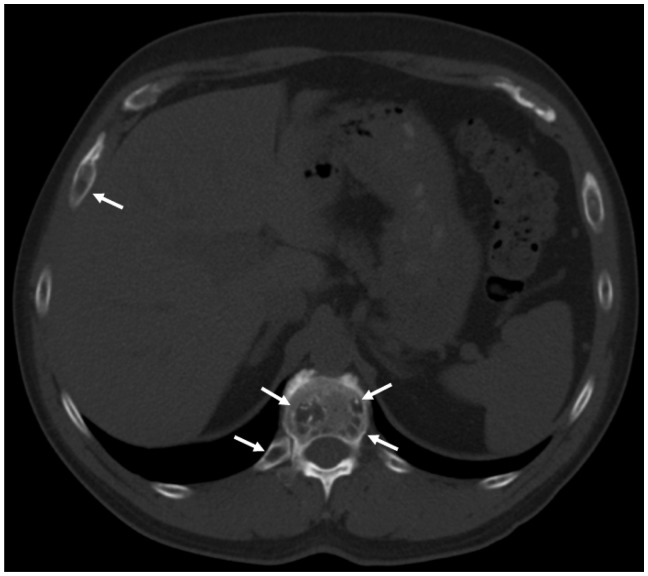
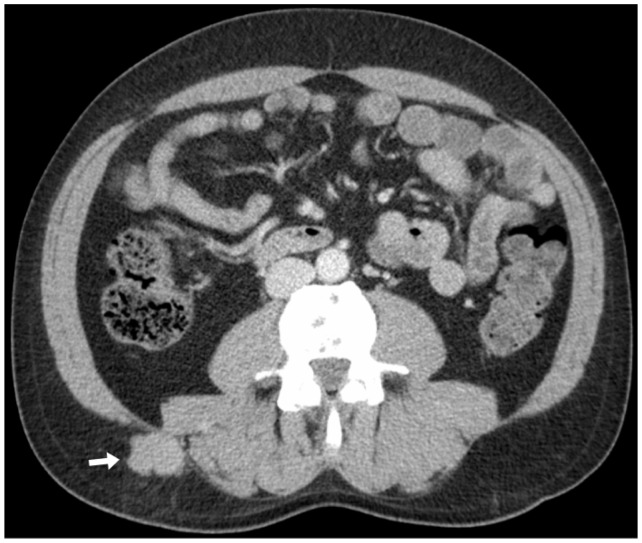
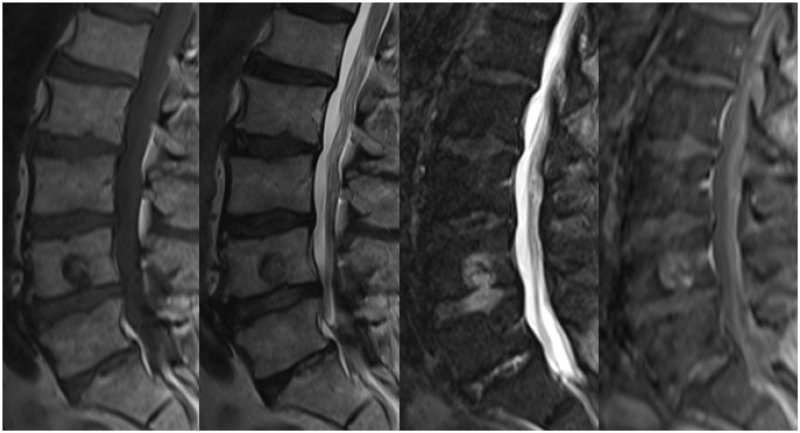
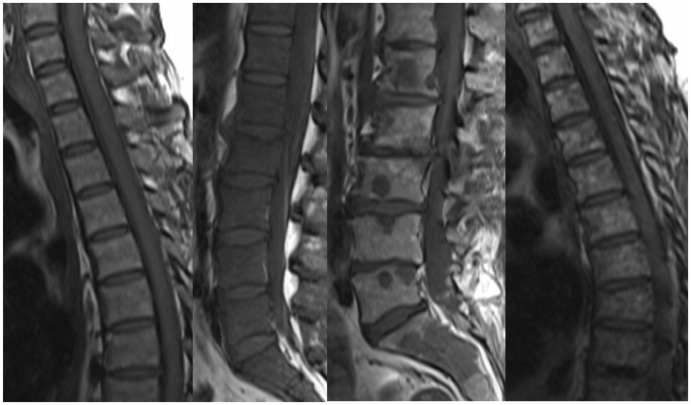
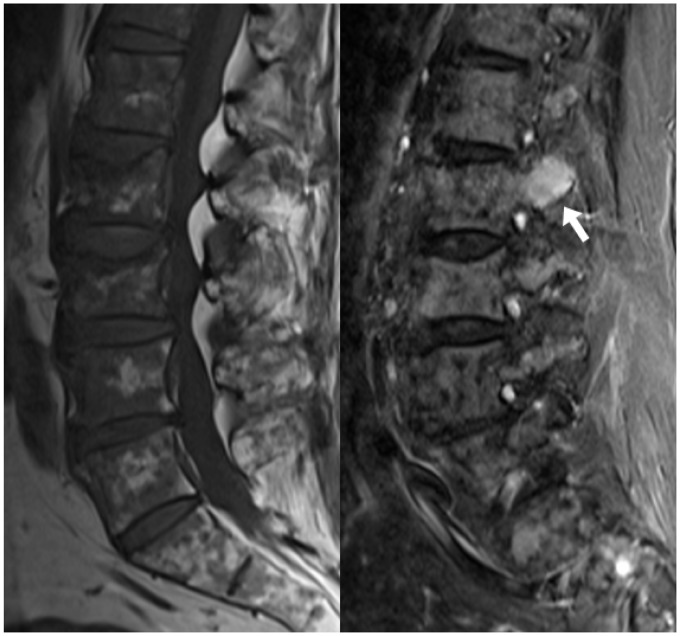
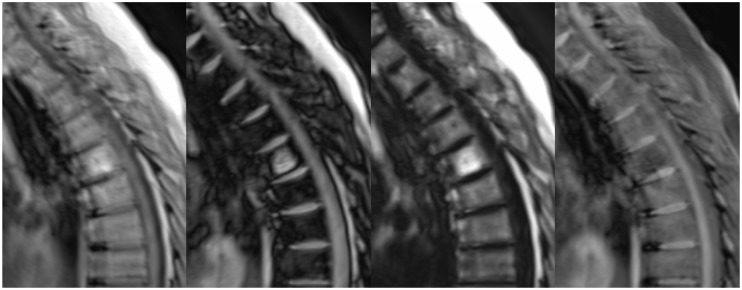
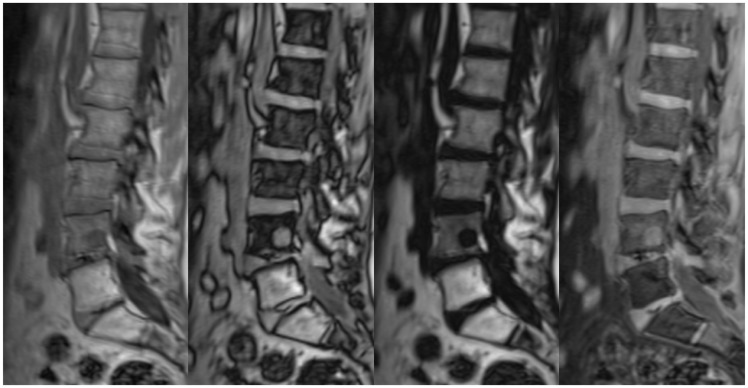
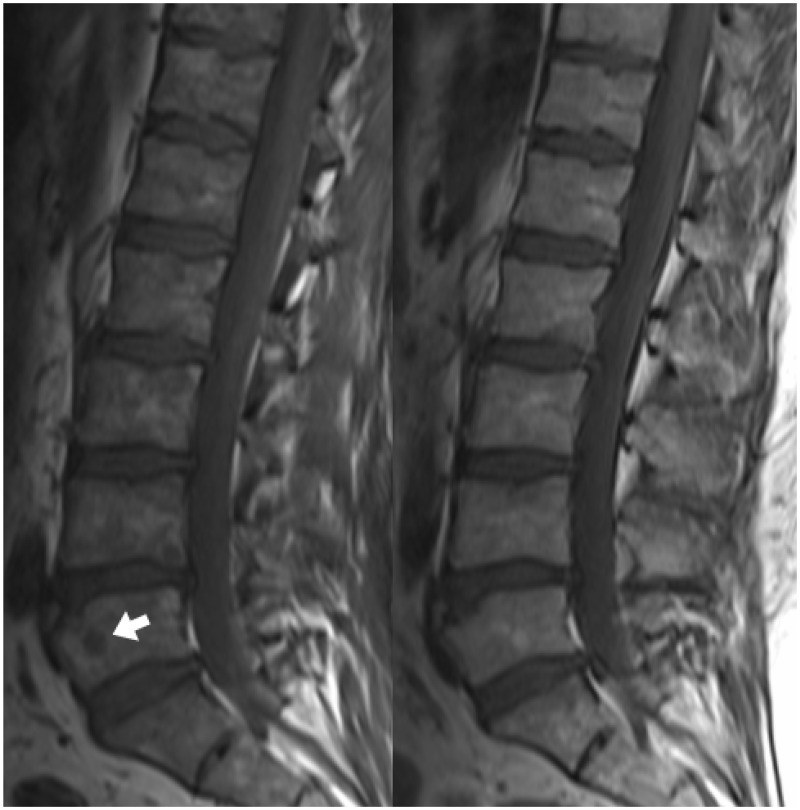
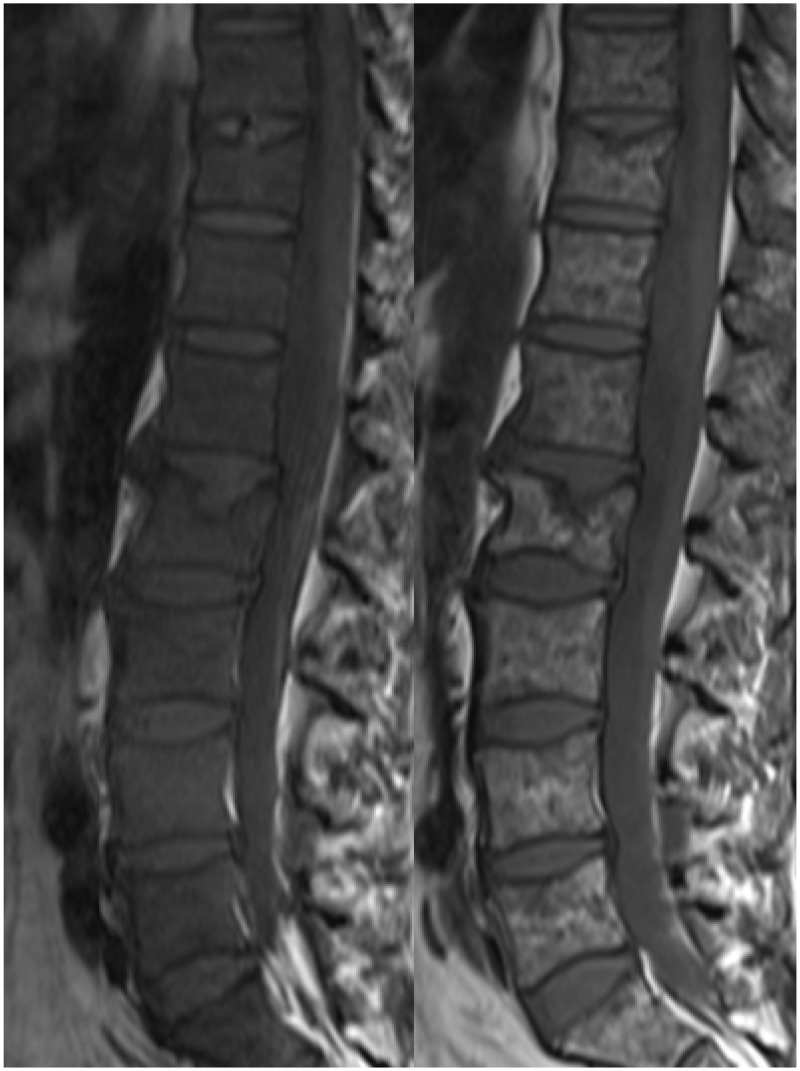
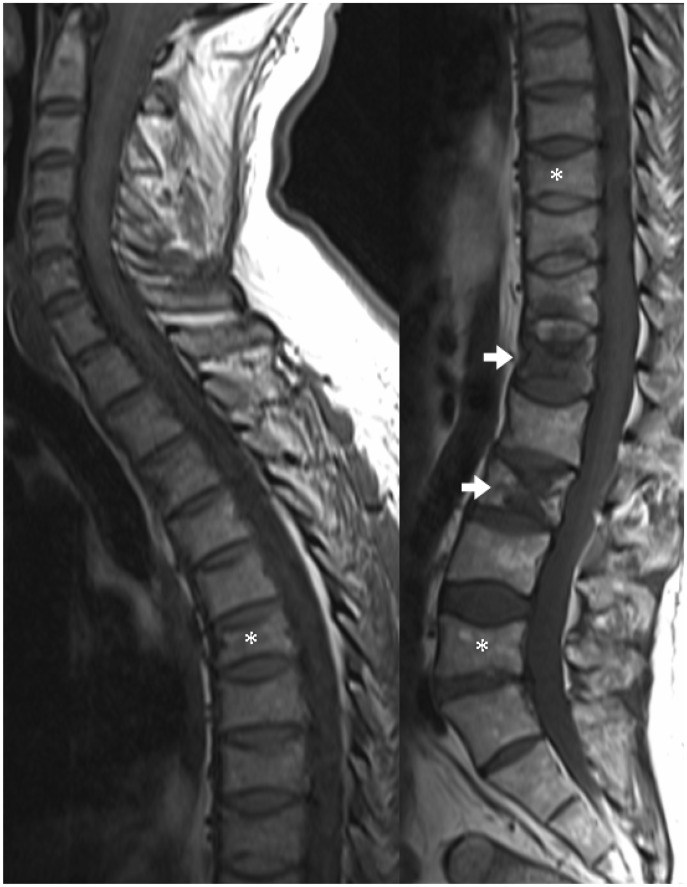
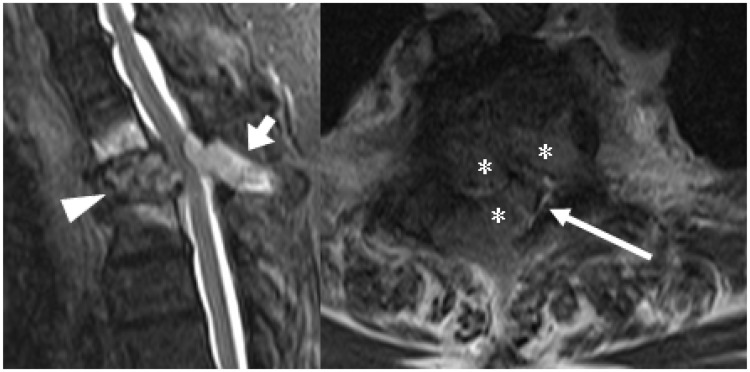
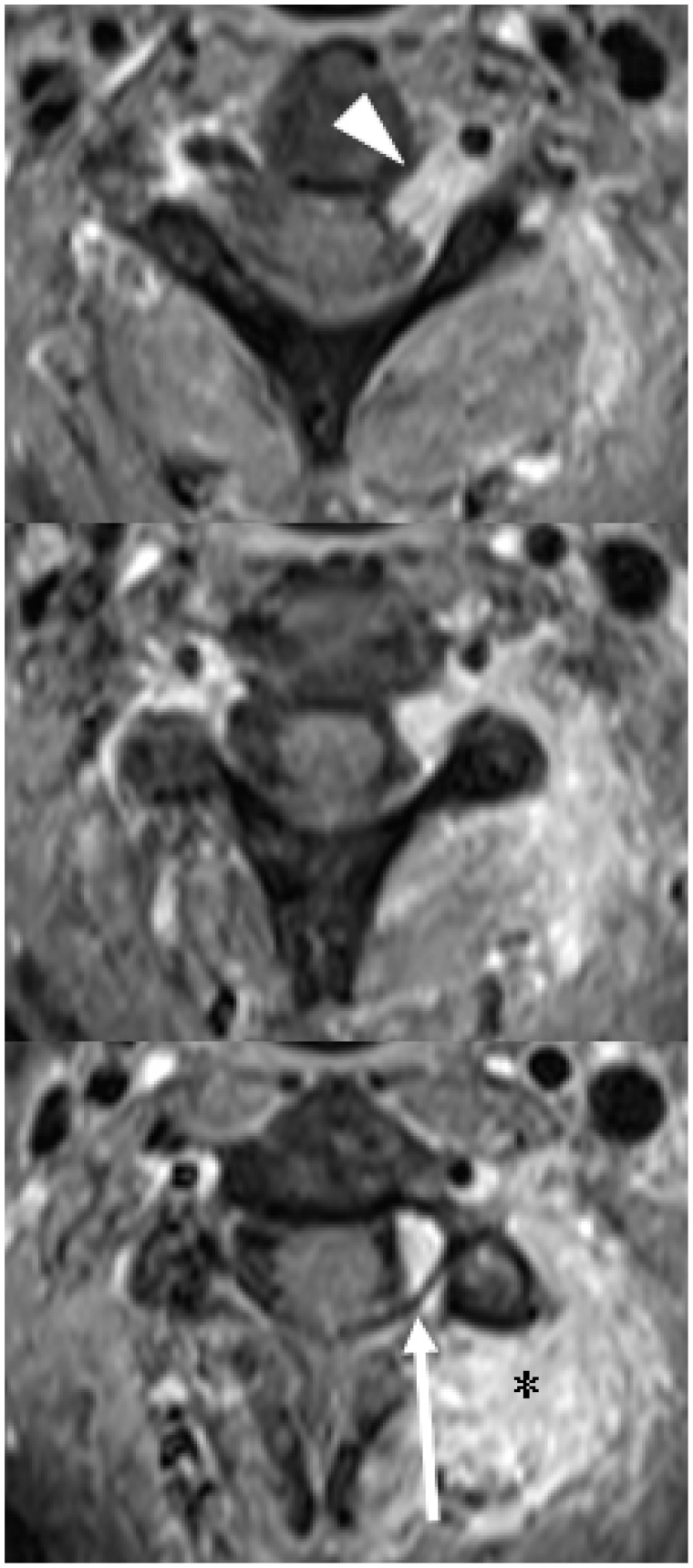
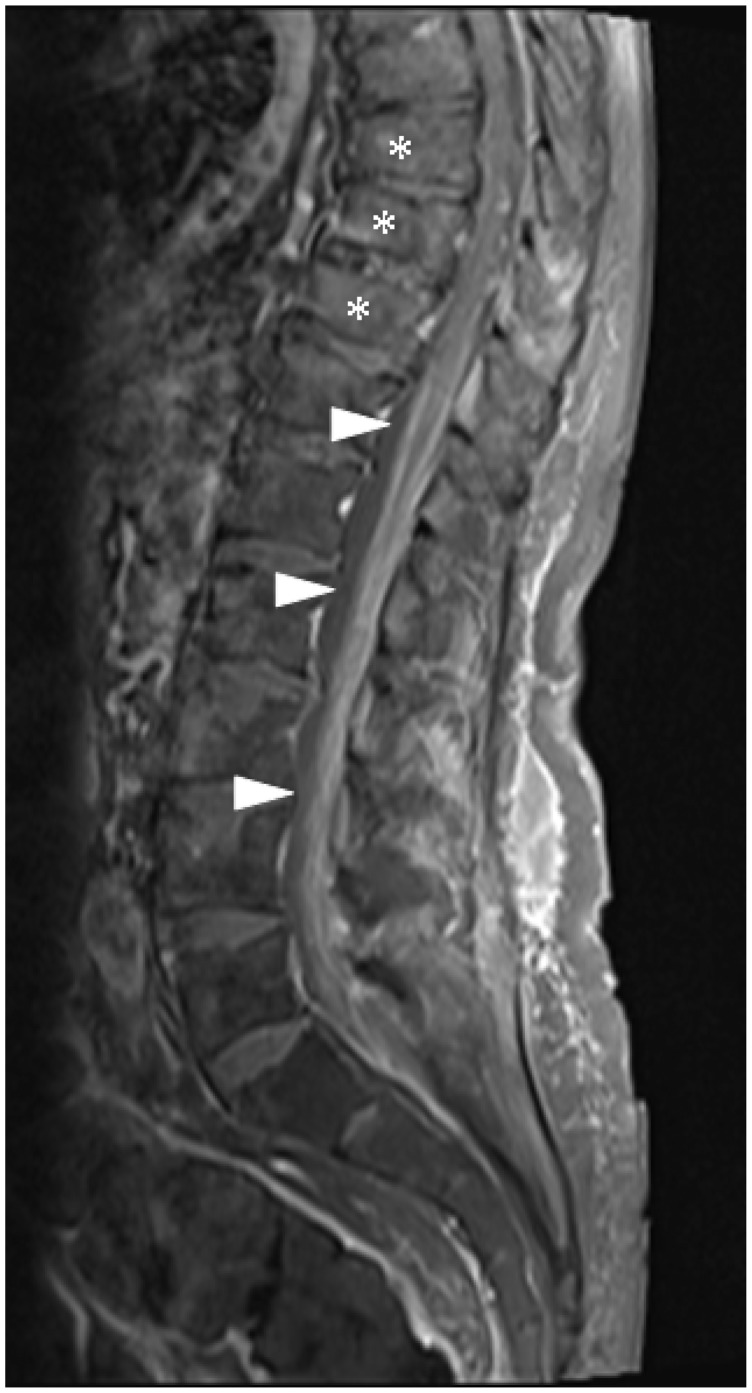
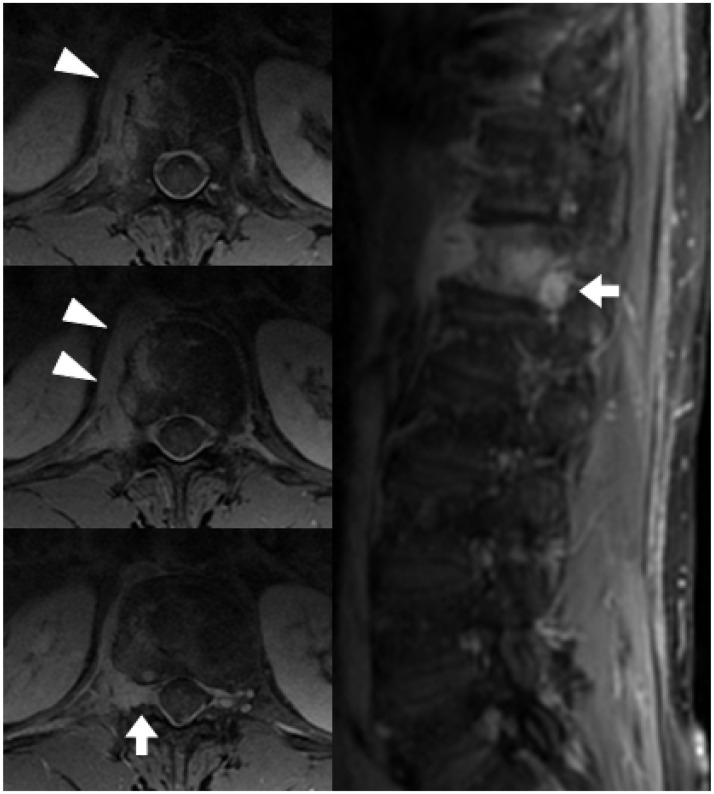
Radiology provides a crucial clinical adjunct in patients with plasma cell disorders, in particular multiple myeloma, and its uses are evolving and expanding. This pictorial review illustrates the role of imaging throughout the patient's clinical course, with specific reference to recently updated international diagnostic criteria. At presentation, imaging optimises characterisation and staging of the plasma-cell disorder, while later in the course of the disease, its roles include the monitoring of disease progression, assessment of post-treatment response and the investigation of clinical deterioration.
Keywords: Magnetic resonance imaging; multiple myeloma; plasmacytoma.
Figures
References
-
- Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol 2014; 15: e538–e548. - PubMed
-
- Bird JM, Owen RG, D’Sa S, et al. Guidelines for the diagnosis and management of multiple myeloma 2011. Br J Haematol 2011; 154: 32–75. - PubMed
-
- Durie BGM, Kyle RA, Belch A, et al. Myeloma management guidelines: a consensus report from the Scientific Advisors of the International Myeloma Foundation. Hematol J 2003; 4: 379–398. - PubMed
-
- Soutar R, Lucraft H, Jackson G, et al. Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma. Br J Haematol 2004; 124: 717–726. - PubMed
-
- Moulopoulos LA, Dimopoulos MA, Weber D, et al. Magnetic resonance imaging in the staging of solitary plasmacytoma of bone. J Clin Oncol 1993; 11: 1311–1315. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
