

Adipocyte hypertrophy-hyperplasia balance contributes to weight loss after bariatric surgery
- PMID: 28425841
- PMCID: PMC5477697
- DOI: 10.1080/21623945.2017.1287639
Adipocyte hypertrophy-hyperplasia balance contributes to weight loss after bariatric surgery
Abstract
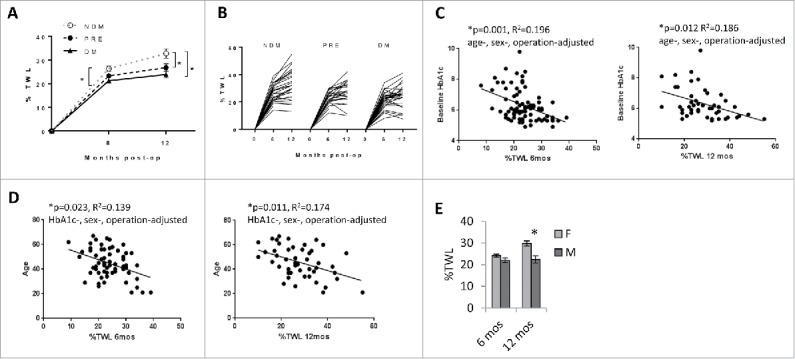
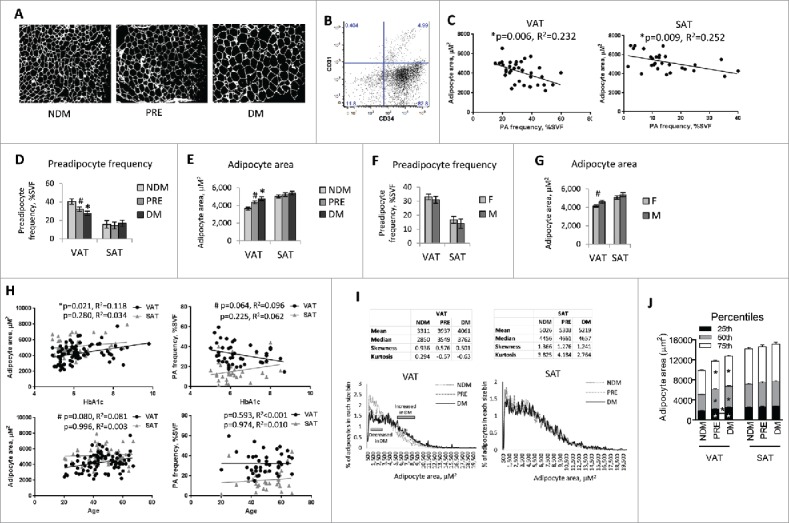
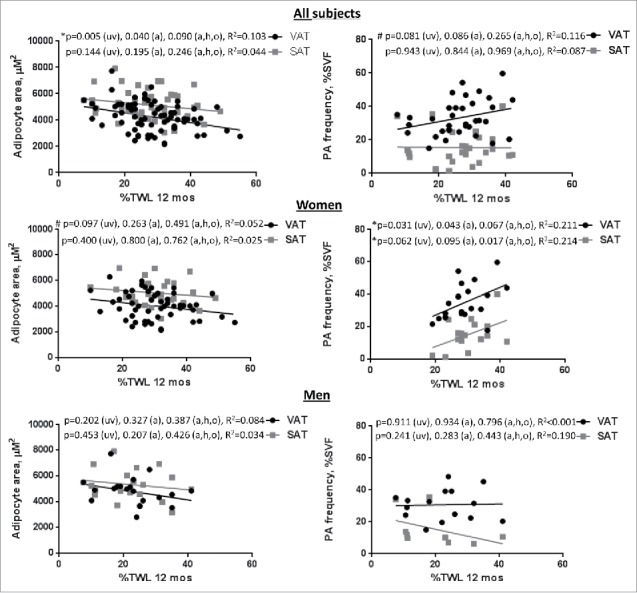
Predictors of weight loss responses are not well-defined. We hypothesized that adipose tissue phenotypic features related to remodeling would be associated with bariatric surgery weight loss responses. Visceral and subcutaneous adipose tissues collected from patients during bariatric surgery were studied with flow cytometry, immunohistochemistry, and QRTPCR, and results correlated with weight loss outcomes. Age, male sex, and a diagnosis of type 2 diabetes were associated with less weight loss. Adipocyte size was increased and preadipocyte frequency was decreased in visceral adipose tissue from diabetic subjects. Decreased adipose tissue preadipocyte frequency was associated with less weight loss in women but not men. These data suggest that phenotypic features of adipose tissue remodeling may predict responses to weight loss interventions.
Keywords: adipose tissue; bariatric surgery; diabetes; hypertrophy; preadipocyte; weight loss.
Figures
References
-
- Brethauer SA, Aminian A, Romero-Talamas H, Batayyah E, Mackey J, Kennedy L, Kashyap SR, Kirwan JP, Rogula T, Kroh M, et al.. Can diabetes be surgically cured? Long-term metabolic effects of bariatric surgery in obese patients with type 2 diabetes mellitus. Ann Surg. 2013; 258(4):628-36; PMID: 24018646 - PMC - PubMed
-
- Agüera Z, García-Ruiz-de-Gordejuela A, Vilarrasa N, Sanchez I, Baño M, Camacho L, Granero R, Jiménez-Murcia S, Virgili N, Lopez-Urdiales R, et al.. Psychological and personality predictors of weight loss and comorbid metabolic changes after bariatric surgery. Eur Eat Disord Rev 2015; 23(6):509-16; PMID: 26377595; https://doi.org/10.1002/erv.2404 - DOI - PubMed
-
- Jurowich C, Thalheimer A, Hartmann D, Bender G, Seyfried F, Germer CT, Wichelmann C. Improvement of type 2 diabetes mellitus (T2DM) after bariatric surgery–who fails in the early postoperative course? Obes Surg 2012; 22(10):1521-6; PMID: 22588846; https://doi.org/10.1007/s11695-012-0676-2 - DOI - PubMed
-
- Ma Y, Pagoto SL, Olendzki BC, Hafner AR, Perugini RA, Mason R, Kelly JJ. Predictors of weight status following laparoscopic gastric bypass. Obes Surg 2006; 16(9):1227-31; PMID: 16989709; https://doi.org/10.1381/096089206778392284 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources