

Southern Tunisia: A still high endemicity area for hepatitis A
- PMID: 28426700
- PMCID: PMC5398567
- DOI: 10.1371/journal.pone.0175887
Southern Tunisia: A still high endemicity area for hepatitis A
Abstract
Background: Hepatitis A (HAV) and E (HEV) viruses are responsible for enterically transmitted hepatitis. Tunisia is reported to be of intermediate endemicity for HAV and of low seroprevalence for HEV; however, data from rural areas of South Tunisia are lacking.
Methods: Sera from 216 asymptomatic pregnant women and from 92 patients with acute hepatitis were collected between October 2014 and November 2015. Total and IgM anti-HAV immunoglobulins and anti-HEV IgG and IgM were investigated. Anti-HAV IgM-positive samples were subjected to RT-PCR targeting the VP1/2A region and sequenced. HEV IgM positive samples and all samples from acute hepatitis patients were assessed for HEV RNA.
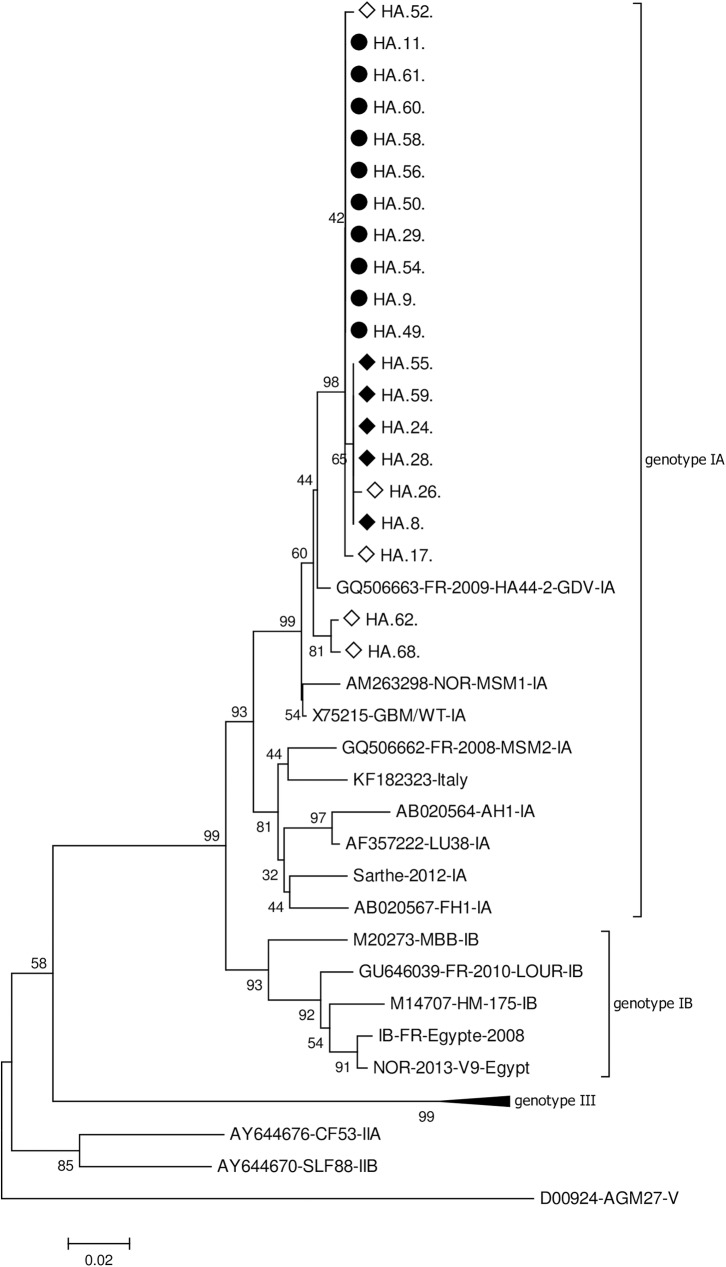
Results: Among pregnant women (mean age 32+/-8), HAV seroprevalence was 98.6%, none presented anti-HAV IgM; HEV seroprevalence was 5.1% and three presented weakly reactive anti-HEV IgM without detectable RNA. Among acute hepatitis patients (mean age 18.5 +/- 14), HEV seroprevalence was 19,5%, none presented anti-HEV IgM, nor HEV RNA. HAV seroprevalence exceeded 90% by age 5 and acute HAV infection was detected in 20 patients (21,7%), younger than patients with other hepatitis causes (9,8 years vs. 20,4 years, p = 0,004); 65% were male. Most acute HAV infections were observed in a coastal area where HAV infections represented 52% of hepatitis etiology. Phylogenetic analysis identified genotype IA strains, clustering close to previously published Tunisian sequences.
Conclusion: The present study confirmed a low HEV endemicity and evidenced a still high level of HAV circulation in Southern Tunisia, suggesting distinct dissemination patterns for these viruses.
Conflict of interest statement
Figures
References
-
- Mohd Hanafiah K, Jacobsen KH, Wiersma ST. Challenges to mapping the health risk of hepatitis A virus infection. Int J Health Geogr. 2011;10:57 PubMed Central PMCID: PMCPMC3210090. doi: 10.1186/1476-072X-10-57 - DOI - PMC - PubMed
-
- WHO position paper on hepatitis A vaccines—June 2012. Wkly Epidemiol Rec. 2012;87(28/29):261–76. - PubMed
-
- Jacobsen KH, Wiersma ST. Hepatitis A virus seroprevalence by age and world region, 1990 and 2005. Vaccine. 2010;28(41):6653–7. doi: 10.1016/j.vaccine.2010.08.037 - DOI - PubMed
-
- Rein DB, Stevens GA, Theaker J, Wittenborn JS, Wiersma ST. The global burden of hepatitis E virus genotypes 1 and 2 in 2005. Hepatology. 2012;55(4):988–97. doi: 10.1002/hep.25505 - DOI - PubMed
-
- Kamar N, Bendall R, Legrand-Abravanel F, Xia NS, Ijaz S, Izopet J, et al. Hepatitis E. Lancet. 2012;379(9835):2477–88. doi: 10.1016/S0140-6736(11)61849-7 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
