

Properties of healthcare teaming networks as a function of network construction algorithms
- PMID: 28426795
- PMCID: PMC5398561
- DOI: 10.1371/journal.pone.0175876
Properties of healthcare teaming networks as a function of network construction algorithms
Abstract
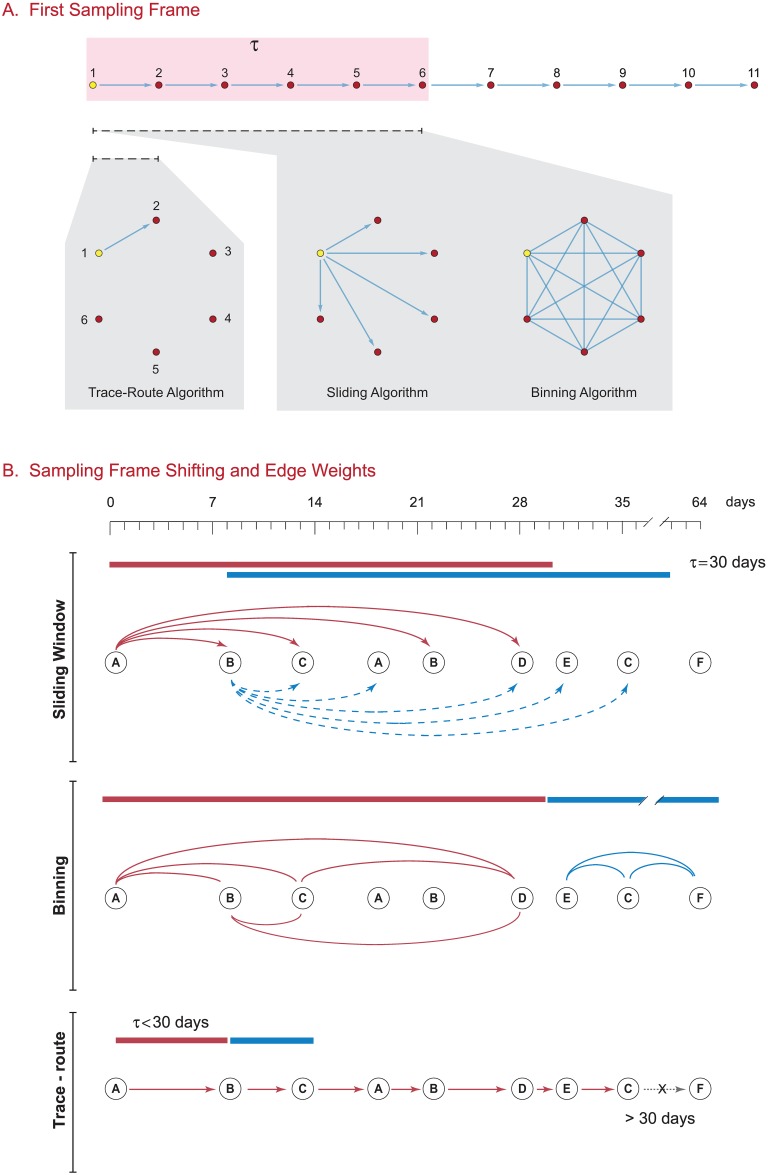
Network models of healthcare systems can be used to examine how providers collaborate, communicate, refer patients to each other, and to map how patients traverse the network of providers. Most healthcare service network models have been constructed from patient claims data, using billing claims to link a patient with a specific provider in time. The data sets can be quite large (106-108 individual claims per year), making standard methods for network construction computationally challenging and thus requiring the use of alternate construction algorithms. While these alternate methods have seen increasing use in generating healthcare networks, there is little to no literature comparing the differences in the structural properties of the generated networks, which as we demonstrate, can be dramatically different. To address this issue, we compared the properties of healthcare networks constructed using different algorithms from 2013 Medicare Part B outpatient claims data. Three different algorithms were compared: binning, sliding frame, and trace-route. Unipartite networks linking either providers or healthcare organizations by shared patients were built using each method. We find that each algorithm produced networks with substantially different topological properties, as reflected by numbers of edges, network density, assortativity, clustering coefficients and other structural measures. Provider networks adhered to a power law, while organization networks were best fit by a power law with exponential cutoff. Censoring networks to exclude edges with less than 11 shared patients, a common de-identification practice for healthcare network data, markedly reduced edge numbers and network density, and greatly altered measures of vertex prominence such as the betweenness centrality. Data analysis identified patterns in the distance patients travel between network providers, and a striking set of teaming relationships between providers in the Northeast United States and Florida, likely due to seasonal residence patterns of Medicare beneficiaries. We conclude that the choice of network construction algorithm is critical for healthcare network analysis, and discuss the implications of our findings for selecting the algorithm best suited to the type of analysis to be performed.
Conflict of interest statement
Figures







References
-
- Almansoori W, Gao S, Jarada TN, Elsheikh AM, Murshed AN, Jida J, et al. Link prediction and classification in social networks and its application in healthcare and systems biology. Network Modeling Analysis in Health Informatics and Bioinformatics. 2012;1(1):27–36. Available from: http://link.springer.com/article/10.1007/s13721-012-0005-7. 10.1007/s13721-012-0005-7 - DOI - DOI
-
- Cunningham FC, Ranmuthugala G, Plumb J, Georgiou A, Westbrook JI, Braithwaite J. Health professional networks as a vector for improving healthcare quality and safety: a systematic review. Quality and Safety in Health Care. 2012;21(3):239–249. Available from: http://qualitysafety.bmj.com/content/21/3/239. 10.1136/bmjqs-2011-000187 - DOI - PMC - PubMed
-
- Gray JE, Davis DA, Pursley DM, Smallcomb JE, Geva A, Chawla NV. Network analysis of team structure in the neonatal intensive care unit. Pediatrics. 2010;125(6):e1460–e1467. Available from: http://pediatrics.aappublications.org/content/125/6/e1460.full-text.pdf. 10.1542/peds.2009-2621 - DOI - PubMed
-
- Gundlapalli A, Ma X, Benuzillo J, Pettey W, Greenberg R, Hales J, et al. Social network analyses of patient-healthcare worker interactions: implications for disease transmission. In: AMIA Annual Symposium Proceedings. American Medical Informatics Association; 2009. p. 213. Available from: http://pubmedcentralcanada.ca/pmcc/articles/PMC2815400/pdf/amia-f2009-21.... - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
