

HER2-Specific Chimeric Antigen Receptor-Modified Virus-Specific T Cells for Progressive Glioblastoma: A Phase 1 Dose-Escalation Trial
- PMID: 28426845
- PMCID: PMC5747970
- DOI: 10.1001/jamaoncol.2017.0184
HER2-Specific Chimeric Antigen Receptor-Modified Virus-Specific T Cells for Progressive Glioblastoma: A Phase 1 Dose-Escalation Trial
Abstract
Importance: Glioblastoma is an incurable tumor, and the therapeutic options for patients are limited.
Objective: To determine whether the systemic administration of HER2-specific chimeric antigen receptor (CAR)-modified virus-specific T cells (VSTs) is safe and whether these cells have antiglioblastoma activity.
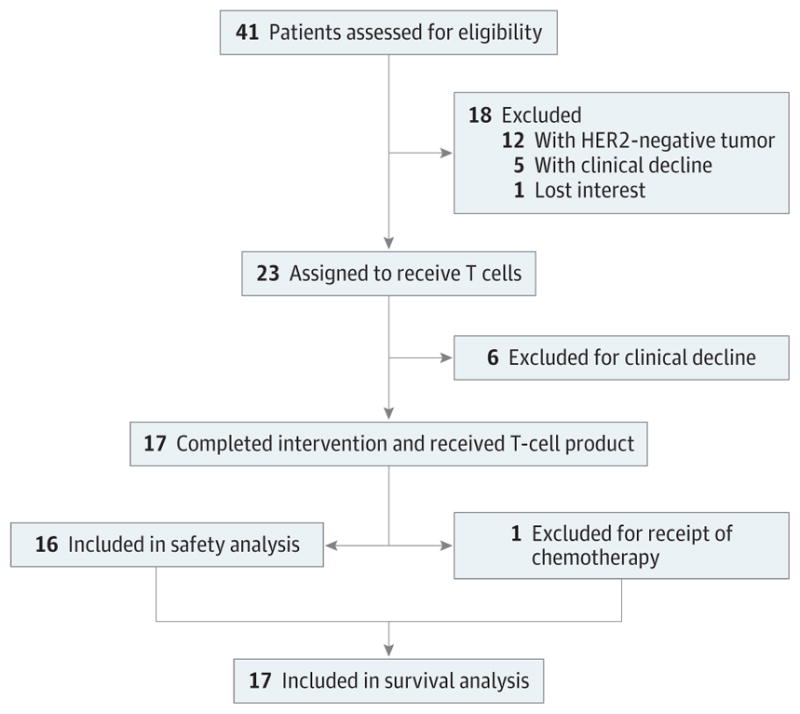
Design, setting, and participants: In this open-label phase 1 dose-escalation study conducted at Baylor College of Medicine, Houston Methodist Hospital, and Texas Children's Hospital, patients with progressive HER2-positive glioblastoma were enrolled between July 25, 2011, and April 21, 2014. The duration of follow-up was 10 weeks to 29 months (median, 8 months).
Interventions: Monotherapy with autologous VSTs specific for cytomegalovirus, Epstein-Barr virus, or adenovirus and genetically modified to express HER2-CARs with a CD28.ζ-signaling endodomain (HER2-CAR VSTs).
Main outcomes and measures: Primary end points were feasibility and safety. The key secondary end points were T-cell persistence and their antiglioblastoma activity.
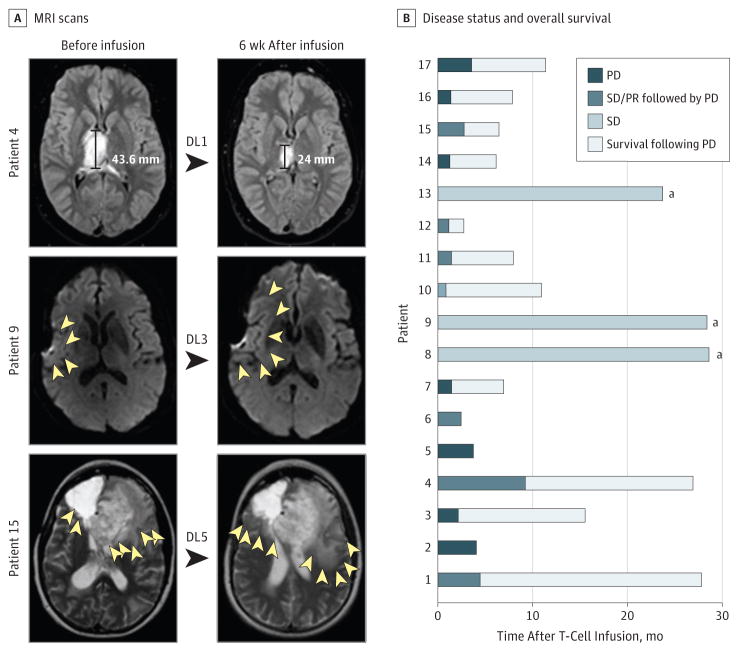
Results: A total of 17 patients (8 females and 9 males; 10 patients ≥18 years [median age, 60 years; range, 30-69 years] and 7 patients <18 years [median age, 14 years; range, 10-17 years]) with progressive HER2-positive glioblastoma received 1 or more infusions of autologous HER2-CAR VSTs (1 × 106/m2 to 1 × 108/m2) without prior lymphodepletion. Infusions were well tolerated, with no dose-limiting toxic effects. HER2-CAR VSTs were detected in the peripheral blood for up to 12 months after the infusion by quantitative real-time polymerase chain reaction. Of 16 evaluable patients (9 adults and 7 children), 1 had a partial response for more than 9 months, 7 had stable disease for 8 weeks to 29 months, and 8 progressed after T-cell infusion. Three patients with stable disease are alive without any evidence of progression during 24 to 29 months of follow-up. For the entire study cohort, median overall survival was 11.1 months (95% CI, 4.1-27.2 months) from the first T-cell infusion and 24.5 months (95% CI, 17.2-34.6 months) from diagnosis.
Conclusions and relevance: Infusion of autologous HER2-CAR VSTs is safe and can be associated with clinical benefit for patients with progressive glioblastoma. Further evaluation of HER2-CAR VSTs in a phase 2b study is warranted as a single agent or in combination with other immunomodulatory approaches for glioblastoma.
Conflict of interest statement
Figures
References
-
- Stupp R, Taillibert S, Kanner AA, et al. Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: a randomized clinical trial. JAMA. 2015;314(23):2535–2543. - PubMed
-
- Pollack IF, Jakacki RI, Butterfield LH, et al. Antigen-specific immune responses and clinical outcome after vaccination with glioma-associated antigen peptides and polyinosinic-polycytidylic acid stabilized by lysine and carboxymethylcellulose in children with newly diagnosed malignant brainstem and nonbrainstem gliomas. J Clin Oncol. 2014;32(19):2050–2058. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
