

Spectacle Wear Among Children in a School-Based Program for Ready-Made vs Custom-Made Spectacles in India: A Randomized Clinical Trial
- PMID: 28426857
- PMCID: PMC5847082
- DOI: 10.1001/jamaophthalmol.2017.0641
Spectacle Wear Among Children in a School-Based Program for Ready-Made vs Custom-Made Spectacles in India: A Randomized Clinical Trial
Abstract
Importance: Uncorrected refractive errors are the most common cause of visual impairment in children despite correction being highly cost-effective.
Objective: To determine whether less expensive ready-made spectacles produce rates of spectacle wear at 3 to 4 months comparable to those of more expensive custom-made spectacles among eligible school-aged children.
Design, setting, and participants: This noninferiority, double-masked, randomized clinical trial recruited children aged 11 to 15 years from January 12 through July 31, 2015, from government schools in urban and periurban areas surrounding Bangalore, India. Follow-up occurred from August 1 through September 31, 2015. Participants met the following eligibility criteria for ready-made spectacles: failed vision screening at the 6/9 level in each eye; refraction was indicated; acuity improved with correction by 2 or more lines in the better-seeing eye; the corrected acuity with the spherical equivalent was not more than 1 line less than with full correction; anisometropia measured less than 1.0 diopter; and an appropriate frame was available.
Interventions: Eligible children were randomized to ready-made or custom-made spectacles.
Main outcomes and measures: Proportion of children wearing their spectacles at unannounced visits 3 to 4 months after the intervention.
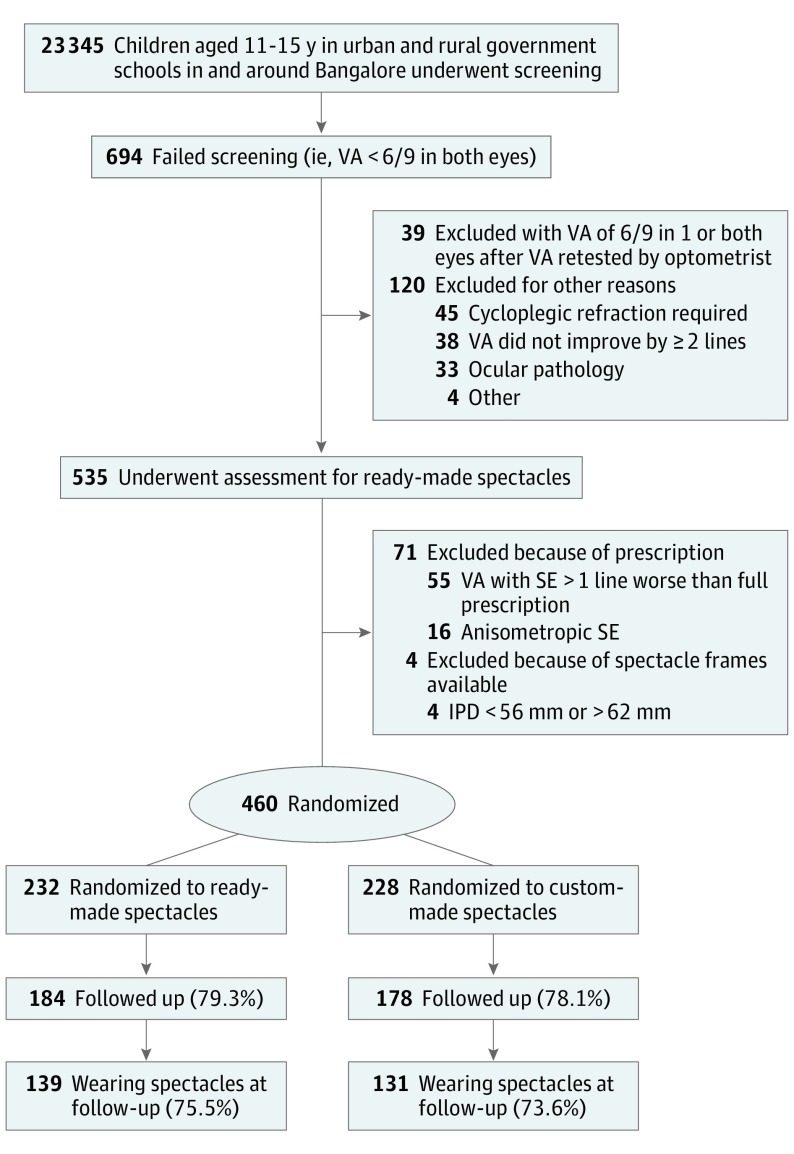
Results: Of 23 345 children aged 11 to 15 years who underwent screening, 694 had visual acuity of less than 6/9 in both eyes, and 535 underwent assessment for eligibility. A total of 460 children (227 female [49.3%] and 233 male [50.7%]; mean [SD] age, 13.4 [1.3] years) were eligible for ready-made spectacles (2.0% undergoing screening and 86.0% undergoing assessment) and were randomized to ready-made (n = 232) or custom-made (n = 228) spectacles. Follow-up rates at 3 to 4 months were similar (184 [79.3%] in the ready-made group and 178 [78.1%] in the custom-made group). Rates of spectacle wear in the 2 arms were similar among 139 of 184 children (75.5%) in the ready-made arm and 131 of 178 children (73.6%) in the custom-made arm (risk difference, 1.8%; 95% CI, -7.1% to 10.8%).
Conclusions and relevance: Most children were eligible for ready-made spectacles, and the proportion wearing ready-made spectacles was not inferior to the proportion wearing custom-made spectacles at 3 to 4 months. These findings suggest that ready-made spectacles could substantially reduce costs for school-based eye health programs in India without compromising spectacle wear, at least in the short term.
Trial registration: isrctn.com Identifier: ISRCTN14715120.
Conflict of interest statement
Figures
References
-
- Robaei D, Huynh SC, Kifley A, Mitchell P. Correctable and non-correctable visual impairment in a population-based sample of 12-year-old Australian children. Am J Ophthalmol. 2006;142(1):112-118. - PubMed
-
- Murthy GVS, Gupta SK, Bachani D. The Principles and Practices of Community Ophthalmology. New Delhi, India: Community Ophthalmology Section, RP Centre, All India Institute of Medical Sciences; 2002.
-
- He M, Huang W, Zheng Y, Huang L, Ellwein LB. Refractive error and visual impairment in school children in rural southern China. Ophthalmology. 2007;114(2):374-382. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
