

Monitoring mandibular movements to detect Cheyne-Stokes Breathing
- PMID: 28427400
- PMCID: PMC5399309
- DOI: 10.1186/s12931-017-0551-8
Monitoring mandibular movements to detect Cheyne-Stokes Breathing
Abstract
Background: The patterns of mandibular movements (MM) during sleep can be used to identify increased respiratory effort periodic large-amplitude MM (LPM), and cortical arousals associated with "sharp" large-amplitude MM (SPM). We hypothesized that Cheyne Stokes breathing (CSB) may be identified by periodic abnormal MM patterns. The present study aims to evaluate prospectively the concordance between CSB detected by periodic MM and polysomnography (PSG) as gold-standard. The present study aims to evaluate prospectively the concordance between CSB detected by periodic MM and polysomnography (PSG) as gold-standard.
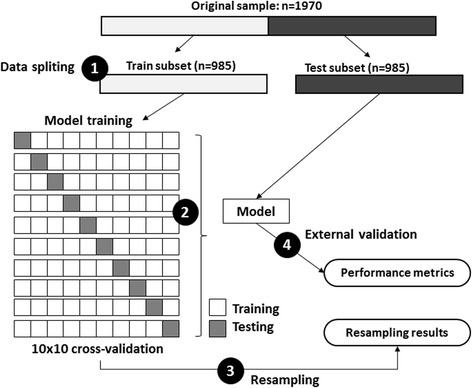
Methods: In 573 consecutive patients attending an in-laboratory PSG for suspected sleep disordered breathing (SDB), MM signals were acquired using magnetometry and scored manually while blinded from the PSG signal. Data analysis aimed to verify the concordance between the CSB identified by PSG and the presence of LPM or SPM. The data were randomly divided into training and validation sets (985 5-min segments/set) and concordance was evaluated using 2 classification models.
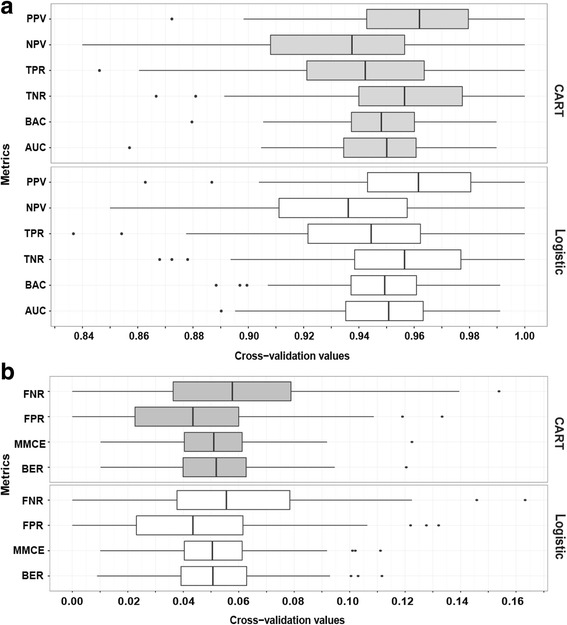
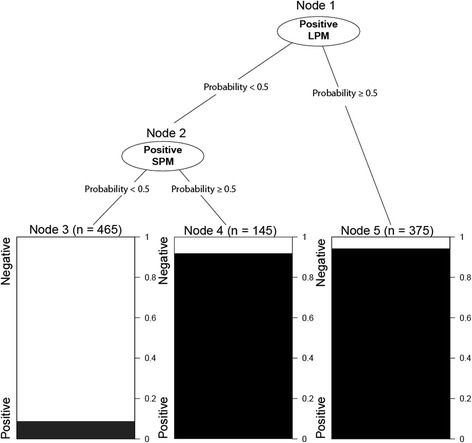
Results: In PSG, 22 patients (mean age ± SD: 65.9 ± 15.0 with a sex ratio M/F of 17/5) had CSB (mean central apnea hourly indice ± SD: 17.5 ± 6.2) from a total of 573 patients with suspected SDB. When tested on independent subset, the classification of CSB based on LPM and SPM is highly accurate (Balanced-accuracy = 0.922, sensitivity = 0.922, specificity = 0.921 and error-rate = 0.078). Logistic models based odds-ratios for CSB in presence of SPM or LPM were 172.43 (95% CI: 88.23-365.04; p < 0.001) and 186.79 (95% CI: 100.48-379.93; p < 0.001), respectively.
Conclusion: CSB in patients with sleep disordered breathing could be accurately identified by a simple magnetometer device recording mandibular movements.
Keywords: Central sleep apnea syndrome; Cheyne Stokes breathing; Polysomnography; Sleep mandibular movements.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
