

Pulmonary hypertension in lymphangioleiomyomatosis: prevalence, severity and the role of carbon monoxide diffusion capacity as a screening method
- PMID: 28427470
- PMCID: PMC5399314
- DOI: 10.1186/s13023-017-0626-0
Pulmonary hypertension in lymphangioleiomyomatosis: prevalence, severity and the role of carbon monoxide diffusion capacity as a screening method
Abstract
Background: Lymphangioleiomyomatosis (LAM) is included within group 5 of the current PH classification (unclear multifactorial mechanisms). However, data regarding the occurrence of PH in LAM are scarce. The aims of the study were to describe the prevalence and characteristics of PH in a large cohort of LAM patients with different levels of severity, and to evaluate the role of echocardiography and carbon monoxide diffusion capacity (DLCO) as screening methods for PH in LAM.
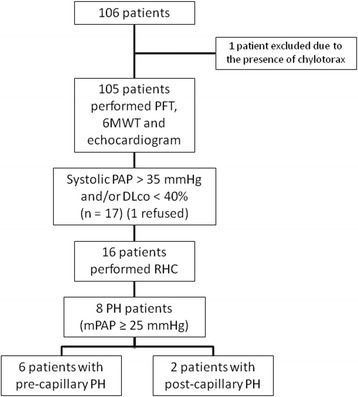
Methods: One hundred five LAM patients underwent transthoracic echocardiography, pulmonary function tests (PFTs) and 6-min walk test (6MWT). Patients with a suspicion of PH on echocardiography, defined by the presence of estimated systolic pulmonary artery pressure (PAP) over 35 mmHg or PFT showing DLco below 40% of the predicted value, underwent right heart catheterisation to confirm the diagnosis of PH.
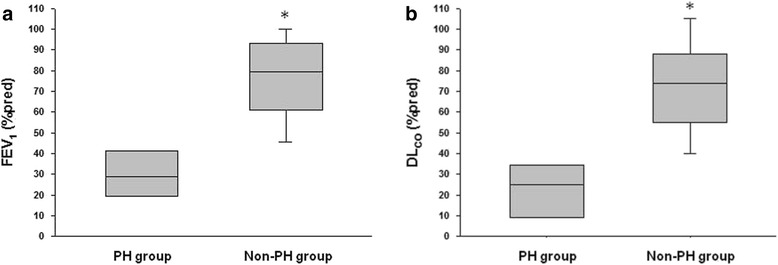
Results: Eight patients (7.6%) had PH confirmed on right heart catheterisation, six patients (5.7%) had a pre-capillary pattern and two patients (1.9%) had a post-capillary profile. Only one patient (1%) had mean PAP over 35 mmHg. Patients with PH had lower FEV1 and DLCO in PFTs and greater oxygen desaturation and dyspnea intensity during 6MWT compared with those without PH. In 63% of the patients with confirmed PH, the right heart catheterisation was performed based only on DLCO result.
Conclusions: The prevalence of PH is low in LAM patients. Pulmonary hypertension in LAM is typically mild and significantly associated with pulmonary parenchymal involvement. Carbon monoxide diffusion capacity significantly improved the identification of PH in LAM patients.
Keywords: Echocardiography; Lymphangioleiomyomatosis; Prevalence; Pulmonary hypertension; Right heart catheterisation.
Figures
Similar articles
-
Clinical characteristics in lymphangioleiomyomatosis-related pulmonary hypertension: an observation on 50 patients.Front Med. 2019 Apr;13(2):259-266. doi: 10.1007/s11684-018-0634-z. Epub 2018 Apr 19. Front Med. 2019. PMID: 29675687
-
[Clinical features of pulmonary hypertension in lymphangioleiomyomatosis].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Aug 12;47(8):746-753. doi: 10.3760/cma.j.cn112147-20240301-00121. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 39069851 Chinese.
-
Pulmonary hypertension in lymphangioleiomyomatosis: characteristics in 20 patients.Eur Respir J. 2012 Sep;40(3):630-40. doi: 10.1183/09031936.00093111. Epub 2012 Feb 23. Eur Respir J. 2012. PMID: 22362861
-
Evolution of Diffusing Capacity of the Lungs for Carbon Monoxide in Lymphangioleiomyomatosis: Historical Perspectives and the Role of Advanced Imaging.Chest. 2025 Jun;167(6):1705-1713. doi: 10.1016/j.chest.2024.11.014. Epub 2024 Nov 21. Chest. 2025. PMID: 39580110 Review.
-
Pulmonary hypertension in chronic lung diseases.J Am Coll Cardiol. 2013 Dec 24;62(25 Suppl):D109-16. doi: 10.1016/j.jacc.2013.10.036. J Am Coll Cardiol. 2013. PMID: 24355635 Review.
Cited by
-
Recent advances in the management of lymphangioleiomyomatosis.F1000Res. 2018 Jun 18;7:F1000 Faculty Rev-758. doi: 10.12688/f1000research.14564.1. eCollection 2018. F1000Res. 2018. PMID: 29946430 Free PMC article. Review.
-
Brazilian Thoracic Association recommendations for the management of lymphangioleiomyomatosis.J Bras Pneumol. 2025 Feb 10;51(1):e20240378. doi: 10.36416/1806-3756/e20240378. eCollection 2025. J Bras Pneumol. 2025. PMID: 39936727 Free PMC article. Review.
-
Haemodynamic definitions and updated clinical classification of pulmonary hypertension.Eur Respir J. 2019 Jan 24;53(1):1801913. doi: 10.1183/13993003.01913-2018. Print 2019 Jan. Eur Respir J. 2019. PMID: 30545968 Free PMC article. Review.
-
Clinical characteristics in lymphangioleiomyomatosis-related pulmonary hypertension: an observation on 50 patients.Front Med. 2019 Apr;13(2):259-266. doi: 10.1007/s11684-018-0634-z. Epub 2018 Apr 19. Front Med. 2019. PMID: 29675687
-
Unmasking a Silent Threat: Improving Pulmonary Hypertension Screening Methods for Interstitial Lung Disease Patients.Medicina (Kaunas). 2023 Dec 28;60(1):58. doi: 10.3390/medicina60010058. Medicina (Kaunas). 2023. PMID: 38256318 Free PMC article. Review.
References
-
- Baldi BG, Freitas CS, Araujo MS, et al. Clinical course and characterization of lymphangioleiomyomatosis in a Brazilian reference centre. Sarc Vasc Diffuse Lung Dis. 2014;31:129–35. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
