

Intentional Percutaneous Laceration of the Anterior Mitral Leaflet to Prevent Outflow Obstruction During Transcatheter Mitral Valve Replacement: First-in-Human Experience
- PMID: 28427597
- PMCID: PMC5579329
- DOI: 10.1016/j.jcin.2017.01.035
Intentional Percutaneous Laceration of the Anterior Mitral Leaflet to Prevent Outflow Obstruction During Transcatheter Mitral Valve Replacement: First-in-Human Experience
Abstract
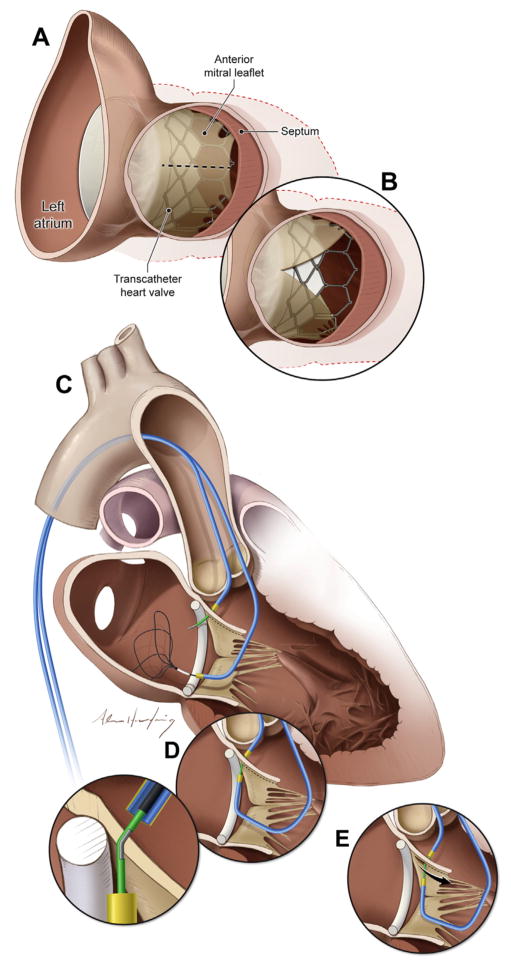
Objectives: This study sought to use a new catheter technique to split the anterior mitral valve leaflet (AML) and prevent iatrogenic left ventricular outflow tract (LVOT) obstruction immediately before transcatheter mitral valve replacement (TMVR).
Background: LVOT obstruction is a life-threatening complication of TMVR, caused by septal displacement of the AML.
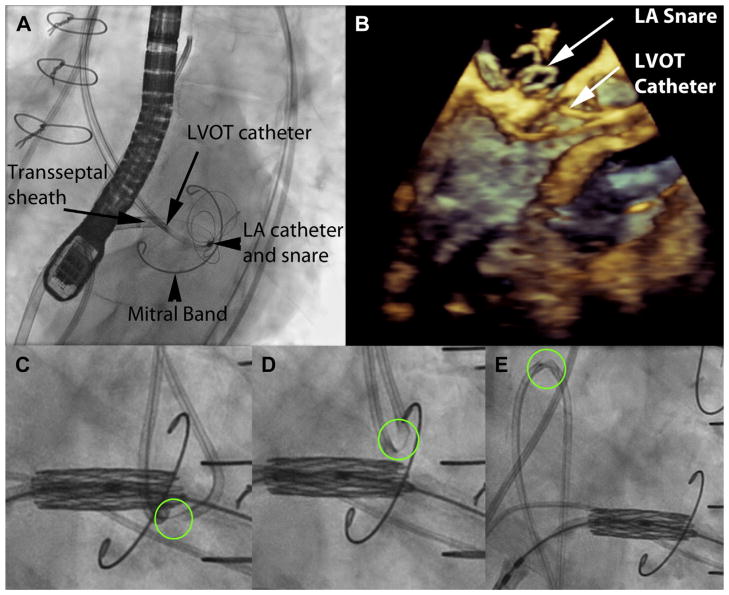
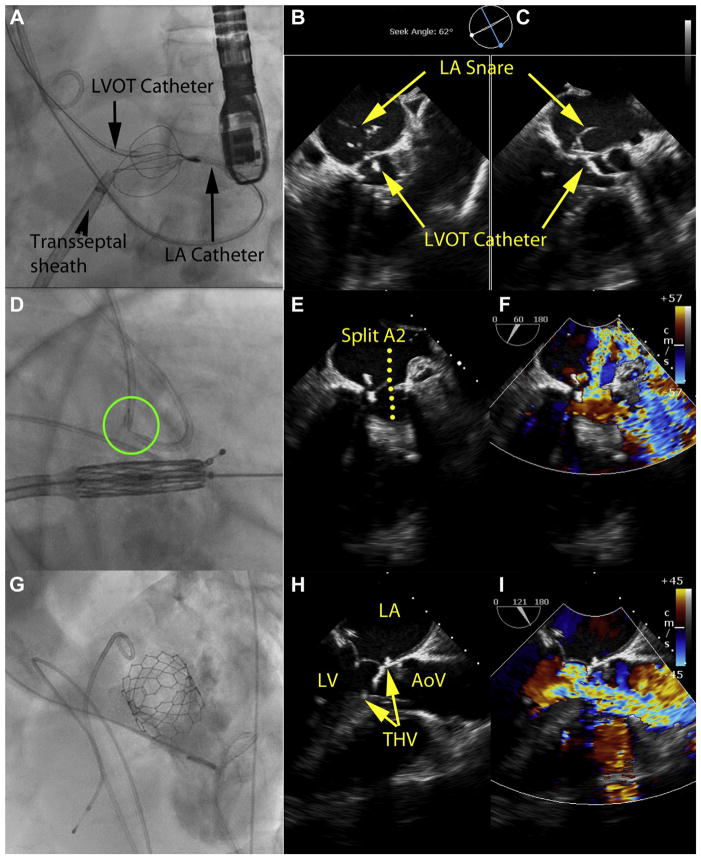
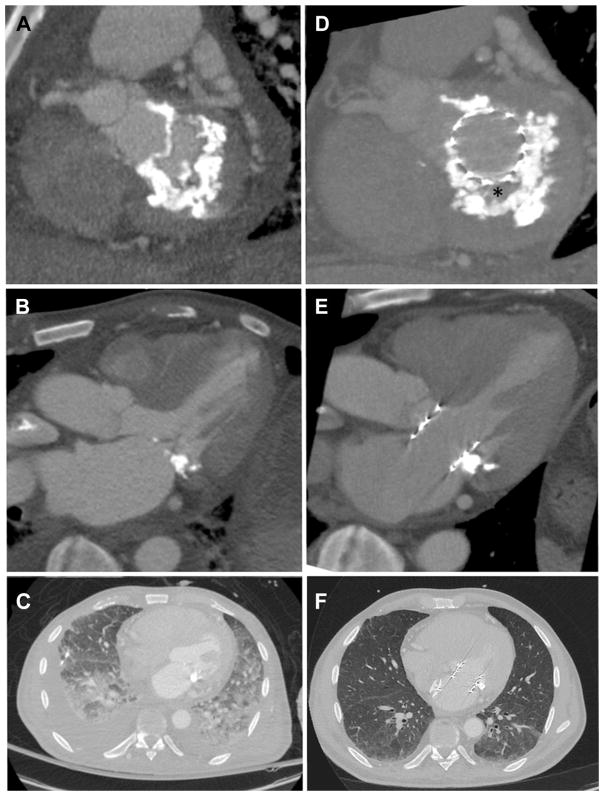
Methods: The procedure was used in patients with severe mitral valve disease and prohibitive surgical risk. Patients either had prior surgical mitral valve ring (n = 3) or band annuloplasty (n = 1) or mitral annular calcification with stenosis (n = 1). Iatrogenic LVOT obstruction or transcatheter heart valve dysfunction was predicted in all based on echocardiography and computed tomography. Transfemoral coronary guiding catheters directed an electrified guidewire across the center and base of the AML toward a snare in the left atrium. The externalized guidewire loop was then electrified to lacerate the AML along the centerline from base to tip, sparing chordae, immediately before transseptal TMVR.
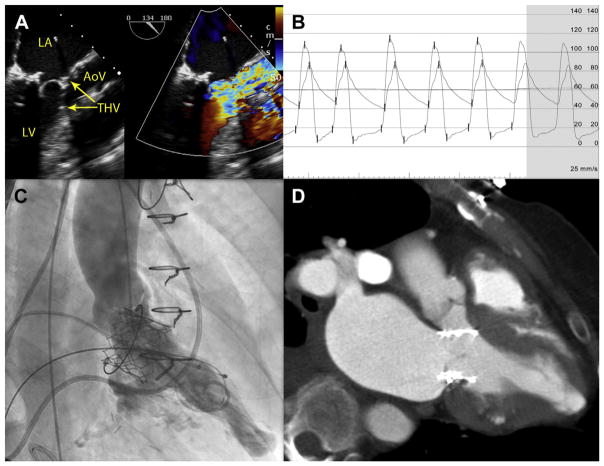
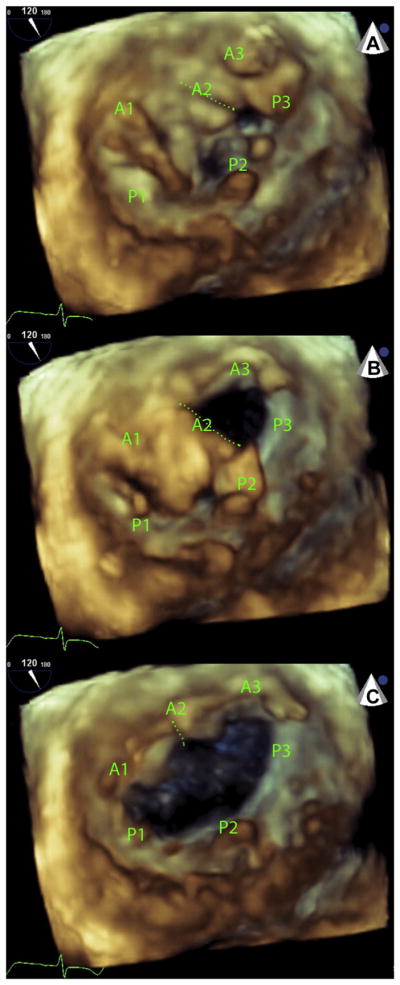
Results: Five patients with prohibitive risk of LVOT obstruction or transcatheter heart valve dysfunction from TMVR successfully underwent LAMPOON, with longitudinal splitting of the A2 scallop of the AML, before valve implantation. Multiplane computed tomography modeling predicted hemodynamic collapse from TMVR assuming an intact AML. However, critical LVOT gradients were not seen following LAMPOON and TMVR. Doppler blood flow was seen across transcatheter heart valve struts that encroached the LVOT, because the AML was split. Transcatheter heart valve function was unimpeded.
Conclusions: This novel catheter technique, which resembles surgical chord-sparing AML resection, may enable TMVR in patients with prohibitive risk of LVOT obstruction or transcatheter heart valve dysfunction.
Keywords: left ventricular outflow tract obstruction; mitral valve; structural heart disease; transcatheter mitral valve replacement; valvular heart disease.
Published by Elsevier Inc.
Figures
References
-
- Anderson RH, Spicer DE, Hlavacek AM, Cook AC, Backer CL. Wilcox’s Surgical Anatomy of the Heart. 4. New York: Cambridge University Press; 2013.
-
- Come PC, Riley MF, Weintraub RM, et al. Dynamic left ventricular outflow tract obstruction when the anterior leaflet is retained at prosthetic mitral valve replacement. Ann Thorac Surg. 1987;43:561–3. - PubMed
-
- Esper E, Ferdinand FD, Aronson S, Karp RB. Prosthetic mitral valve replacement: late complications after native valve preservation. Ann Thorac Surg. 1997;63:541–3. - PubMed
-
- Bapat V, Pirone F, Kapetanakis S, Rajani R, Niederer S. Factors influencing left ventricular outflow tract obstruction following a mitral valve-in-valve or valve-in-ring procedure, part 1. Catheter Cardiovasc Interv. 2015;86:747–60. - PubMed
-
- Hamid NB, Khalique OK, Monaghan MJ, et al. Transcatheter valve implantation in failed surgically inserted bioprosthesis: review and practical guide to echocardiographic imaging in valve-in-valve procedures. J Am Coll Cardiol Img. 2015;8:960–79. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
