

In Vivo Detection of EGFRvIII in Glioblastoma via Perfusion Magnetic Resonance Imaging Signature Consistent with Deep Peritumoral Infiltration: The φ-Index
- PMID: 28428190
- PMCID: PMC5559313
- DOI: 10.1158/1078-0432.CCR-16-1871
In Vivo Detection of EGFRvIII in Glioblastoma via Perfusion Magnetic Resonance Imaging Signature Consistent with Deep Peritumoral Infiltration: The φ-Index
Abstract
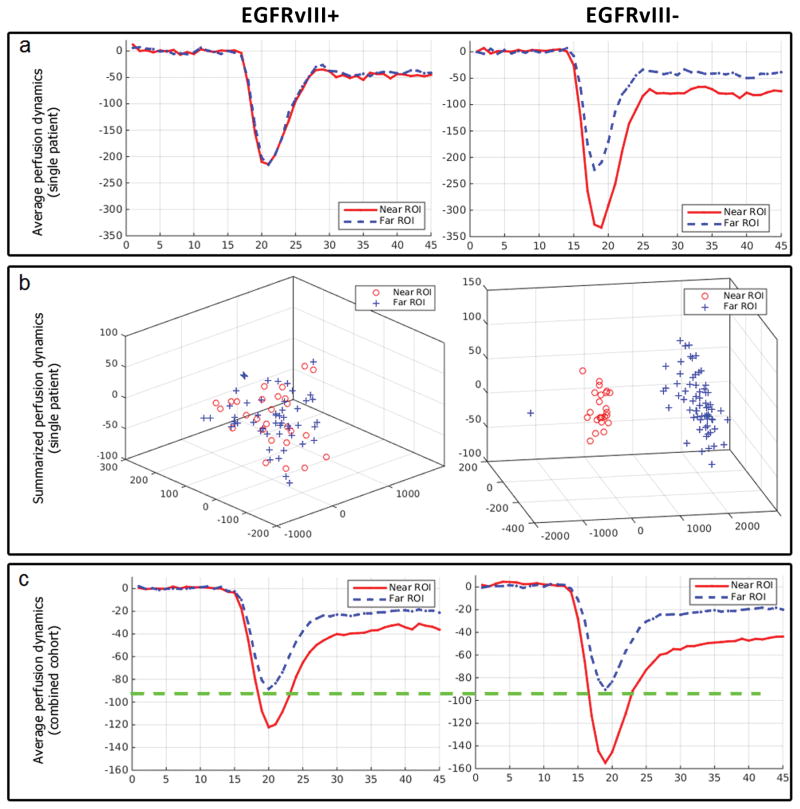
Purpose: The epidermal growth factor receptor variant III (EGFRvIII) mutation has been considered a driver mutation and therapeutic target in glioblastoma, the most common and aggressive brain cancer. Currently, detecting EGFRvIII requires postoperative tissue analyses, which are ex vivo and unable to capture the tumor's spatial heterogeneity. Considering the increasing evidence of in vivo imaging signatures capturing molecular characteristics of cancer, this study aims to detect EGFRvIII in primary glioblastoma noninvasively, using routine clinically acquired imaging.Experimental Design: We found peritumoral infiltration and vascularization patterns being related to EGFRvIII status. We therefore constructed a quantitative within-patient peritumoral heterogeneity index (PHI/φ-index), by contrasting perfusion patterns of immediate and distant peritumoral edema. Application of φ-index in preoperative perfusion scans of independent discovery (n = 64) and validation (n = 78) cohorts, revealed the generalizability of this EGFRvIII imaging signature.Results: Analysis in both cohorts demonstrated that the obtained signature is highly accurate (89.92%), specific (92.35%), and sensitive (83.77%), with significantly distinctive ability (P = 4.0033 × 10-10, AUC = 0.8869). Findings indicated a highly infiltrative-migratory phenotype for EGFRvIII+ tumors, which displayed similar perfusion patterns throughout peritumoral edema. Contrarily, EGFRvIII- tumors displayed perfusion dynamics consistent with peritumorally confined vascularization, suggesting potential benefit from extensive peritumoral resection/radiation.Conclusions: This EGFRvIII signature is potentially suitable for clinical translation, since obtained from analysis of clinically acquired images. Use of within-patient heterogeneity measures, rather than population-based associations, renders φ-index potentially resistant to inter-scanner variations. Overall, our findings enable noninvasive evaluation of EGFRvIII for patient selection for targeted therapy, stratification into clinical trials, personalized treatment planning, and potentially treatment-response evaluation. Clin Cancer Res; 23(16); 4724-34. ©2017 AACR.
©2017 American Association for Cancer Research.
Conflict of interest statement
Figures





References
-
- Johnson DR, O’Neill BP. Glioblastoma survival in the United States before and during the temozolomide era. Journal of Neuro-Oncology. 2011;107:359–64. - PubMed
-
- Aum DJ, Kim DH, Beaumont TL, Leuthardt EC, Dunn GP, Kim AH. Molecular and cellular heterogeneity: the hallmark of glioblastoma. Neurosurg Focus. 2014;37:E11. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
