

Therapeutic experience of 289 elderly patients with biliary diseases
- PMID: 28428722
- PMCID: PMC5385409
- DOI: 10.3748/wjg.v23.i13.2424
Therapeutic experience of 289 elderly patients with biliary diseases
Abstract
Aim: To present clinical characteristics, diagnosis and treatment strategies in elderly patients with biliary diseases.
Methods: A total of 289 elderly patients with biliary diseases were enrolled in this study. The clinical data relating to these patients were collected in our hospital from June 2013 to May 2016. Patient age, disease type, coexisting diseases, laboratory examinations, surgical methods, postoperative complications and therapeutic outcomes were analyzed.
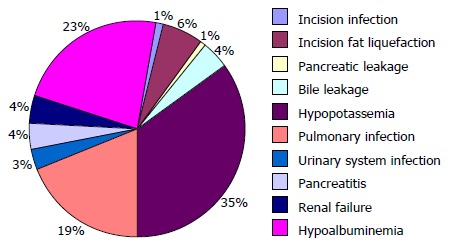
Results: The average age of the 289 patients with biliary diseases was 73.9 ± 8.5 years (range, 60-102 years). One hundred and thirty-one patients (45.3%) had one of 10 different biliary diseases, such as gallbladder stones, common bile duct stones, and cholangiocarcinoma. The remaining patients (54.7%) had two types of biliary diseases. One hundred and seventy-nine patients underwent 9 different surgical treatments, including pancreaticoduodenectomy, radical resection of hilar cholangiocarcinoma and laparoscopic cholecystectomy. Ten postoperative complications occurred with an incidence of 39.3% (68/173), and hypopotassemia showed the highest incidence (33.8%, 23/68). One hundred and sixteen patients underwent non-surgical treatments, including anti-infection, symptomatic and supportive treatments. The cure rate was 97.1% (168/173) in the surgical group and 87.1% (101/116) in the non-surgical group. The difference between these two groups was statistically significant (χ2 = 17.227, P < 0.05).
Conclusion: Active treatment of coexisting diseases, management of indications and surgical opportunities, appropriate selection of surgical procedures, improvements in perioperative therapy, and timely management of postoperative complications are key factors in enhancing therapeutic efficacy in elderly patients with biliary diseases.
Keywords: Biliary diseases; Elderly patients; Non-operative treatment; Surgical treatment.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that there are no conflicts of interest related to this study.
Figures



Similar articles
-
One hundred consecutive hepatobiliary resections for biliary hilar malignancy: preoperative blood donation, blood loss, transfusion, and outcome.Surgery. 2005 Feb;137(2):148-55. doi: 10.1016/j.surg.2004.06.006. Surgery. 2005. PMID: 15674194
-
Endoscopic management of postoperative bile leaks.Hepatobiliary Pancreat Dis Int. 2006 May;5(2):273-7. Hepatobiliary Pancreat Dis Int. 2006. PMID: 16698590
-
Impact of gallbladder status on the outcome in patients with retained bile duct stones treated with extracorporeal shockwave lithotripsy.Endoscopy. 2002 Aug;34(8):624-7. doi: 10.1055/s-2002-33243. Endoscopy. 2002. PMID: 12173082
-
[Laparoscopic cholecystectomy causing injury to biliary tracts. Analysis of the results of 26,440 operations in Hungary].Orv Hetil. 1996 May 5;137(18):955-63. Orv Hetil. 1996. PMID: 8649757 Review. Hungarian.
-
Hotspots and difficulties of biliary surgery in older patients.Chin Med J (Engl). 2023 May 5;136(9):1037-1046. doi: 10.1097/CM9.0000000000002589. Chin Med J (Engl). 2023. PMID: 37052140 Free PMC article. Review.
Cited by
-
Elderly persons with acute pancreatitis - specifics of the clinical course of the disease.Clin Interv Aging. 2018 Dec 21;14:33-41. doi: 10.2147/CIA.S188520. eCollection 2019. Clin Interv Aging. 2018. PMID: 30613137 Free PMC article.
-
Emergency one-stage endoscopic treatment in the older adults with acute cholangitis with choledocholithiasis: a propensity score-matched analysis.Eur Geriatr Med. 2025 Sep 2. doi: 10.1007/s41999-025-01296-8. Online ahead of print. Eur Geriatr Med. 2025. PMID: 40897944
-
Current Status of Surgical Treatment of Biliary Diseases in Elderly Patients in China.Chin Med J (Engl). 2018 Aug 5;131(15):1873-1876. doi: 10.4103/0366-6999.237405. Chin Med J (Engl). 2018. PMID: 30058588 Free PMC article. No abstract available.
-
Therapeutic experience of an 89-year-old high-risk patient with incarcerated cholecystolithiasis: A case report and literature review.World J Clin Cases. 2020 Oct 26;8(20):4908-4916. doi: 10.12998/wjcc.v8.i20.4908. World J Clin Cases. 2020. PMID: 33195660 Free PMC article.
-
Comparison of the efficacy of laparoscopic primary closure of the common bile duct and T-tube drainage in the treatment of choledocholithiasis in elderly patients.BMC Geriatr. 2025 Jul 28;25(1):549. doi: 10.1186/s12877-025-06210-2. BMC Geriatr. 2025. PMID: 40721750 Free PMC article.
References
-
- Zhang ZM, Song MM, Liu Z, Zhang C, Liu LM, Yu HW, Wan BJ, Liu ZX, Zhu MW, Wei WP, et al. Clinical effect and analysis of laparoscopic cholecystectomy in elderly patients with acute calculous cholecystitis. Zhonghua Puwaike Shoushuxue Zazhi (Electronic Edition) 2016;10:466–468.
-
- Pavlidis TE, Marakis GN, Symeonidis N, Psarras K, Ballas K, Rafailidis S, Sakantamis AK. Considerations concerning laparoscopic cholecystectomy in the extremely elderly. J Laparoendosc Adv Surg Tech A. 2008;18:56–60. - PubMed
-
- Tucker JJ, Yanagawa F, Grim R, Bell T, Ahuja V. Laparoscopic cholecystectomy is safe but underused in the elderly. Am Surg. 2011;77:1014–1020. - PubMed
-
- Wagner D, Büttner S, Kim Y, Gani F, Xu L, Margonis GA, Amini N, Kamel IR, Pawlik TM. Clinical and morphometric parameters of frailty for prediction of mortality following hepatopancreaticobiliary surgery in the elderly. Br J Surg. 2016;103:e83–e92. - PubMed
-
- Makary MA, Segev DL, Pronovost PJ, Syin D, Bandeen-Roche K, Patel P, Takenaga R, Devgan L, Holzmueller CG, Tian J, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010;210:901–908. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
