

Surgical Strategy and Techniques for Low-Profile Dorsal Plating in Treating Dorsally Displaced Unstable Distal Radius Fractures
- PMID: 28428920
- PMCID: PMC5397302
- DOI: 10.1055/s-0036-1593763
Surgical Strategy and Techniques for Low-Profile Dorsal Plating in Treating Dorsally Displaced Unstable Distal Radius Fractures
Abstract
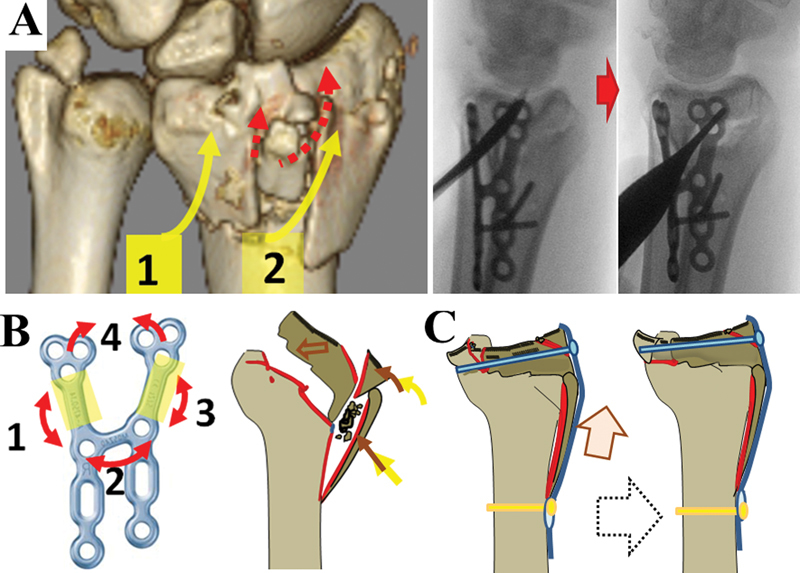
Background The low-profile dorsal locking plating (DLP) technique is useful for treating dorsally comminuted intra-articular distal radius fractures; however, due to the complications associated with DLP, the technique is not widely used. Methods A retrospective review of 24 consecutive cases treated with DLP were done. Results All cases were classified into two types by surgical strategy according to the fracture pattern. In type 1, there is a volar fracture line distal to the watershed line in the dorsally displaced fragment, and this type is treated by H-framed DLP. In type 2, the displaced dorsal die-punch fragment is associated with a minimally displaced styloid shearing fracture or a transverse volar fracture line. We found that the die-punch fragment was reduced by the buttress effect of small l-shaped DLP after stabilization of the styloid shearing for the volar segment by cannulated screws from radial styloid processes. At 6 months after surgery, outcomes were good or excellent based on the modified Mayo wrist scores with no serious complications except one case. The mean range of motion of each type was as follows: the palmar flexion was 50, 65 degrees, dorsiflexion was 70, 75 degrees, supination was 85, 85 degrees, and pronation was 80, 80 degrees; in type 1 and 2, respectively. Conclusion DLP is a useful technique for the treatment of selected cases of dorsally displaced, comminuted intra-articular fractures of the distal radius with careful soft tissue coverage.
Keywords: dorsally displaced distal radius fractures; fracture type; indication and clinical results; low-profile dorsal locking plates; surgical strategy and technique.
Conflict of interest statement
Figures




Similar articles
-
Volar fixation of dorsally displaced distal radius fractures using the 2.4-mm locking compression plates.J Hand Surg Am. 2005 Jul;30(4):743-9. doi: 10.1016/j.jhsa.2005.03.006. J Hand Surg Am. 2005. PMID: 16039367
-
Functional outcome and complications after volar plating for dorsally displaced, unstable fractures of the distal radius.J Hand Surg Am. 2006 Mar;31(3):359-65. doi: 10.1016/j.jhsa.2005.10.010. J Hand Surg Am. 2006. PMID: 16516728
-
Complications following internal fixation of unstable distal radius fracture with a palmar locking-plate.J Orthop Trauma. 2007 May;21(5):316-22. doi: 10.1097/BOT.0b013e318059b993. J Orthop Trauma. 2007. PMID: 17485996
-
Are Volar Locking Plates Superior to Percutaneous K-wires for Distal Radius Fractures? A Meta-analysis.Clin Orthop Relat Res. 2015 Sep;473(9):3017-27. doi: 10.1007/s11999-015-4347-1. Epub 2015 May 16. Clin Orthop Relat Res. 2015. PMID: 25981715 Free PMC article. Review.
-
The use of dorsal distraction plating for severely comminuted distal radius fractures: A review and comparison to volar plate fixation.Injury. 2019 Jun;50 Suppl 1:S50-S55. doi: 10.1016/j.injury.2019.03.052. Epub 2019 Apr 6. Injury. 2019. PMID: 31040029 Review.
Cited by
-
Early Mobilization Versus Splinting After Surgical Management of Distal Radius Fractures.Dtsch Arztebl Int. 2020 Jun 26;117(26):445-451. doi: 10.3238/arztebl.2020.0445. Dtsch Arztebl Int. 2020. PMID: 32897182 Free PMC article. Clinical Trial.
-
A new classification and its value evaluation for intermediate column fractures of the distal radius.J Orthop Surg Res. 2018 Sep 3;13(1):221. doi: 10.1186/s13018-018-0925-8. J Orthop Surg Res. 2018. PMID: 30176895 Free PMC article.
-
The Die Punch Fragment: Analysis of Fragment Geometry and Need for Fixation.J Hand Microsurg. 2020 May 12;14(2):127-131. doi: 10.1055/s-0040-1712328. eCollection 2022 Apr. J Hand Microsurg. 2020. PMID: 35983286 Free PMC article.
-
Minimally Invasive Fixation with Dorsal Suspension Button and Volar Plate in Distal Radius Fractures with Dorsal Die Punch Fragments: A Preliminary Study.J Wrist Surg. 2022 Jul 12;12(2):161-169. doi: 10.1055/s-0042-1749161. eCollection 2023 Apr. J Wrist Surg. 2022. PMID: 36926206 Free PMC article.
-
Treatment of unstable extra-articular distal radius fractures using locked volar plating and percutaneous pinning without external fixation.Int J Burns Trauma. 2020 Aug 15;10(4):113-120. eCollection 2020. Int J Burns Trauma. 2020. PMID: 32934865 Free PMC article.
References
-
- Dy C J, Wolfe S W, Jupiter J B, Blazar P E, Ruch D S, Hanel D P. Distal radius fractures: strategic alternatives to volar plate fixation. Instr Course Lect. 2014;63:27–37. - PubMed
-
- Tyllianakis M E, Panagopoulos A M, Saridis A. Long-term results of dorsally displaced distal radius fractures treated with the pi-plate: is hardware removal necessary? Orthopedics. 2011;34(7):e282–e286. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
