

Improved systemic treatment for early breast cancer improves cure rates, modifies metastatic pattern and shortens post-metastatic survival: 35-year results from the Munich Cancer Registry
- PMID: 28429102
- PMCID: PMC11819226
- DOI: 10.1007/s00432-017-2428-0
Improved systemic treatment for early breast cancer improves cure rates, modifies metastatic pattern and shortens post-metastatic survival: 35-year results from the Munich Cancer Registry
Abstract
Purpose: Systemic therapies (ATHs) in early breast cancer have improved the survival of breast cancer (BC) patients in recent decades. The magnitude of the changes in overall, metastasis-free (MFS) and post-metastatic (PMS) survival and in the metastasis (MET) pattern will be described.
Patient and methods: We analysed 60,227 patients with a diagnosis of T-N-M0 BC between 1978 and 2013 and 11,983 patients with metastases (MET) in the Munich Cancer Registry. Patients will be divided into four time periods to identify relationships between BC and METs. Survival was estimated using Kaplan-Meier curves, and Cox proportional hazards models were used to explore the impact of the BC subtype and MET status on survival with the time periods as surrogate markers for ATH evolution.
Results: During the observation period, 5-year relative survival has improved from 80.3 to 93.6% with an adjusted hazard ratio of 0.54 (P < 0.0001). Successful implementation of ATH has changed the MET pattern. The percentage of liver and CNS METs has more than doubled, the rate of lung METs remains stable, and the rate of bone METs has been reduced by approximately 50%. MFS has been prolonged with a hazard ratio 0.75 (P < 0.0001), but PMS has declined (hazard ratio 1.36; P < 0.0001); however, effects of adjuvant and palliative treatments cannot be separated. These results do not contradict improvements in advanced BC and do not suggest alterations of MET tumour biology by ATH.
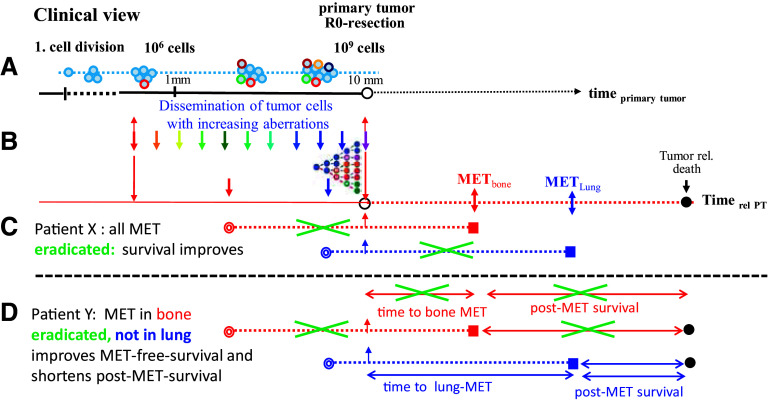
Conclusions: Over the past three decades, ATHs have dramatically improved patient survival after BC diagnosis-most likely, by eradicating prevalent micro-METs; as a result, the MET pattern has changed. Eradicating only a portion of the first METs results in delaying the onset of subsequent MET, which leads to an apparently paradoxical effect: an extension of the MET-free interval and a reduction in PMS.
Keywords: Breast cancer; Metastasis; Metastasis organs; Survival; Time trend.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


Similar articles
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
-
Bisphosphonates and other bone agents for breast cancer.Cochrane Database Syst Rev. 2017 Oct 30;10(10):CD003474. doi: 10.1002/14651858.CD003474.pub4. Cochrane Database Syst Rev. 2017. PMID: 29082518 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
Cited by
-
Machine Learning-Based Prediction of Distant Recurrence in Invasive Breast Carcinoma Using Clinicopathological Data: A Cross-Institutional Study.Cancers (Basel). 2023 Aug 3;15(15):3960. doi: 10.3390/cancers15153960. Cancers (Basel). 2023. PMID: 37568776 Free PMC article.
-
Gaps in Care and Support for Patients With Advanced Breast Cancer: A Report From the Advanced Breast Cancer Global Alliance.JCO Glob Oncol. 2021 Jun;7:976-984. doi: 10.1200/GO.21.00045. JCO Glob Oncol. 2021. PMID: 34156869 Free PMC article.
-
Improved survival in metastatic breast cancer: results from a 20-year study involving 1033 women treated at a single comprehensive cancer center.J Cancer Res Clin Oncol. 2020 Jun;146(6):1559-1566. doi: 10.1007/s00432-020-03184-z. Epub 2020 Mar 18. J Cancer Res Clin Oncol. 2020. PMID: 32189107 Free PMC article.
-
Demographic and Clinical Features of Patients with Metastatic Breast Cancer: A Retrospective Multicenter Registry Study of the Turkish Oncology Group.Cancers (Basel). 2023 Mar 8;15(6):1667. doi: 10.3390/cancers15061667. Cancers (Basel). 2023. PMID: 36980554 Free PMC article.
-
Impact of high dose radiotherapy for breast tumor in locoregionally uncontrolled stage IV breast cancer: a need for a risk-stratified approach.Radiat Oncol. 2023 Oct 11;18(1):168. doi: 10.1186/s13014-023-02357-7. Radiat Oncol. 2023. PMID: 37821947 Free PMC article. Review.
References
-
- Curado M, Edwards B, Shin H, Storm H, Ferlay J, Heanue M et al (2007) Cancer Incidence in five continents, vol. IX. IARC Scientific Publication No. 160
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
