

Carfilzomib-lenalidomide-dexamethasone vs lenalidomide-dexamethasone in relapsed multiple myeloma by previous treatment
- PMID: 28430175
- PMCID: PMC5436074
- DOI: 10.1038/bcj.2017.31
Carfilzomib-lenalidomide-dexamethasone vs lenalidomide-dexamethasone in relapsed multiple myeloma by previous treatment
Abstract
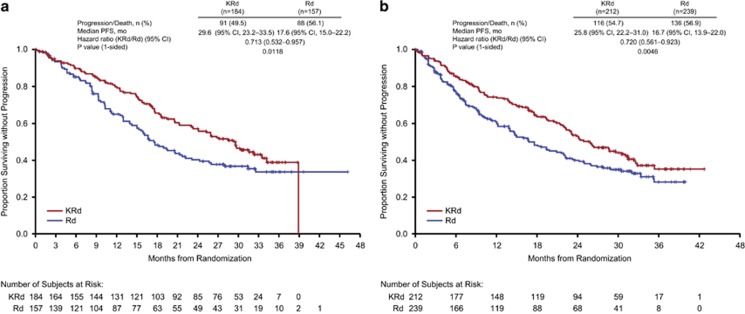
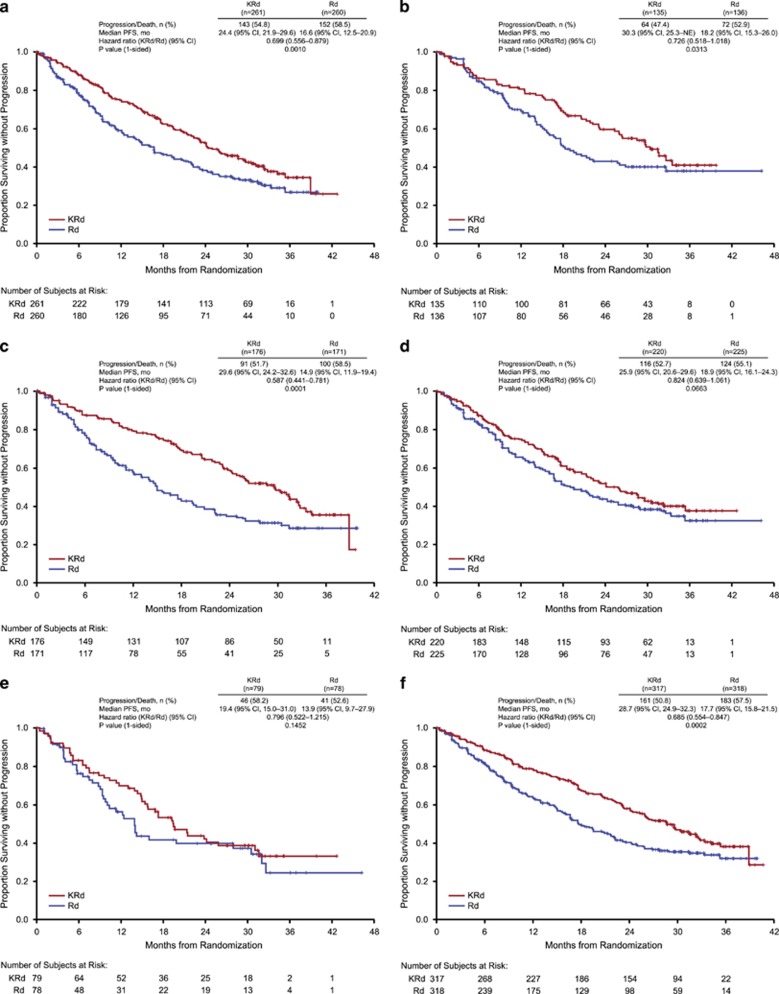
Carfilzomib, a proteasome inhibitor, is approved as monotherapy and in combination with dexamethasone or lenalidomide-dexamethasone (Rd) for relapsed or refractory multiple myeloma. The approval of carfilzomib-lenalidomide-dexamethasone (KRd) was based on results from the randomized, phase 3 study ASPIRE (NCT01080391), which showed KRd significantly improved progression-free survival (PFS) vs Rd (median 26.3 vs 17.6 months; hazard ratio (HR)=0.690; P=0.0001). This subgroup analysis of ASPIRE evaluated KRd vs Rd by number of previous lines of therapy and previous exposure to bortezomib, thalidomide or lenalidomide. Treatment with KRd led to a 12-month improvement in median PFS vs Rd after first relapse (HR 0.713) and a 9-month improvement after ⩾2 previous lines of therapy (HR 0.720). Treatment with KRd led to an approximate 8-month improvement vs Rd in median PFS in bortezomib-exposed patients (HR 0.699), a 15-month improvement in thalidomide-exposed patients (HR 0.587) and a 5-month improvement in lenalidomide-exposed patients (HR 0.796). Objective response and complete response or better rates were higher with KRd vs Rd, irrespective of previous treatment. KRd had a favorable benefit-risk profile and should be considered an appropriate treatment option for patients with 1 or ⩾2 previous lines of therapy and those previously exposed to bortezomib, thalidomide or lenalidomide.
Conflict of interest statement
MAD has served as a consultant for and has received honoraria from Celgene, Onyx, Janssen, Novartis and Amgen. AKS has received honoraria from Amgen, Celgene and Onyx; and has served in a consulting or advisory role for Celgene, Janssen and Takeda. TM has served as a consultant for Novartis, Janssen-Cilag, BMS and Takeda. IS has served as consultant for and received research funding from and holds membership on Board of Directors or advisory committee of Celgene and Janssen-Cilag. AO has served as consultant for and has served as a speakers' bureau participant for Celgene, Janssen and Amgen. RH has served as a consultant for and received honoraria from Celgene, Janssen and Amgen. LR has received honoraria from Celgene and Janssen. DS has received honoraria from and has served as speakers' bureau participant for Celgene, Takeda, BMS, Amgen, Novartis and Merck. RN has served as consultant for and has served as a speakers' bureau participant for Celgene, Millennium and Onyx. AJ has served as consultant or on advisory boards for, has received research funding from, has received honoraria from Onyx (Amgen), Celgene, BMS, Janssen-Cilag, Karyopharm, Inc., Millennium (Takeda), Sanofi Aventis and SkylineDx. JS-M has had a consulting or advisory role with BMS, Celgene, Janssen, Millennium, Merck Sharp & Dohme, Novartis and Onyx. HL has served as a speakers' bureau participant for Amgen, BMS, Celgene, Novartis and Takeda; and has received study support from Takeda. SR and SA report equity ownership and employment with Amgen/Onyx. PM has served as consultant for and has received honoraria from Novartis, Janssen, Celgene, Millennium and Onyx. AP is an employee of Takeda; has received honoraria from and served as consultant for Amgen, Novartis, Bristol-Myers Squibb, Genmab A/S, Celgene, Janssen-Cilag, Takeda, Sanofi Aventis and Merck; has received research funding from Amgen, Novartis, Bristol-Myers Squibb, Genmab A/S, Celgene, Janssen-Cilag, Takeda, Sanofi Aventis, Merck and Binding Site; and participated in a speakers' bureau for Bristol-Myers Squibb. The remaining authors declare no conflict of interest.
Figures
References
-
- Dimopoulos MA, Richardson PG, Moreau P, Anderson KC. Current treatment landscape for relapsed and/or refractory multiple myeloma. Nat Rev Clin Oncol 2015; 12: 42–54. - PubMed
-
- Moreau P, San Miguel J, Ludwig H, Schouten H, Mohty M, Dimopoulos M et al. ESMO Guidelines Working Group. multiple myeloma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2013; 24(Suppl 6): vi133–vi137. - PubMed
-
- Song X, Cong Z, Wilson K. Real world treatment patterns and comorbidities and disease-related complications in patients with multiple myeloma in the United States. Curr Med Res Opin 2016; 32: 95–103. - PubMed
-
- National Comprehensive Care Network (2016). Clinical Practice Guidelines in Oncology. Multiple Myeloma.
-
- Kumar SK, Therneau TM, Gertz MA, Lacy MQ, Dispenzieri A, Rajkumar SV et al. Clinical course of patients with relapsed multiple myeloma. Mayo Clin Proc 2004; 79: 867–874. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
