

Lymphovascular invasion is a high risk factor for stage I/II colorectal cancer: a systematic review and meta-analysis
- PMID: 28430621
- PMCID: PMC5542293
- DOI: 10.18632/oncotarget.15425
Lymphovascular invasion is a high risk factor for stage I/II colorectal cancer: a systematic review and meta-analysis
Abstract
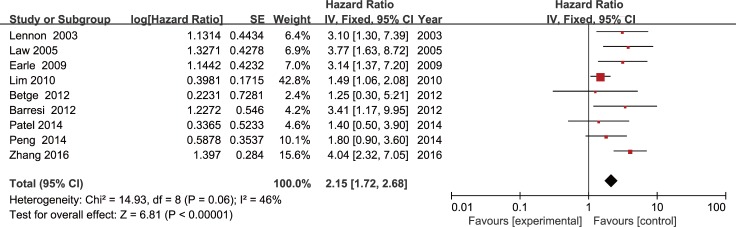
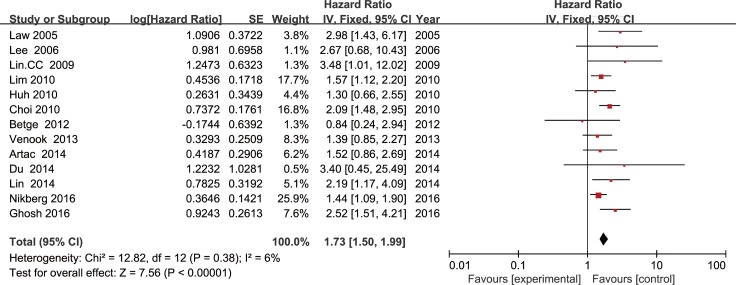
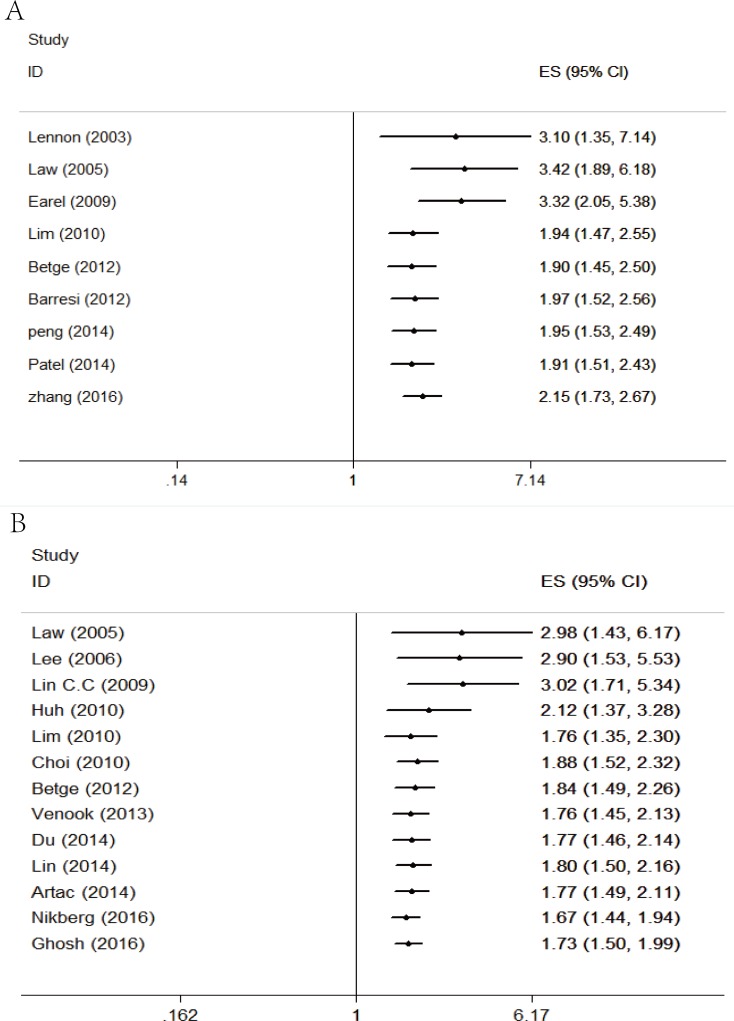
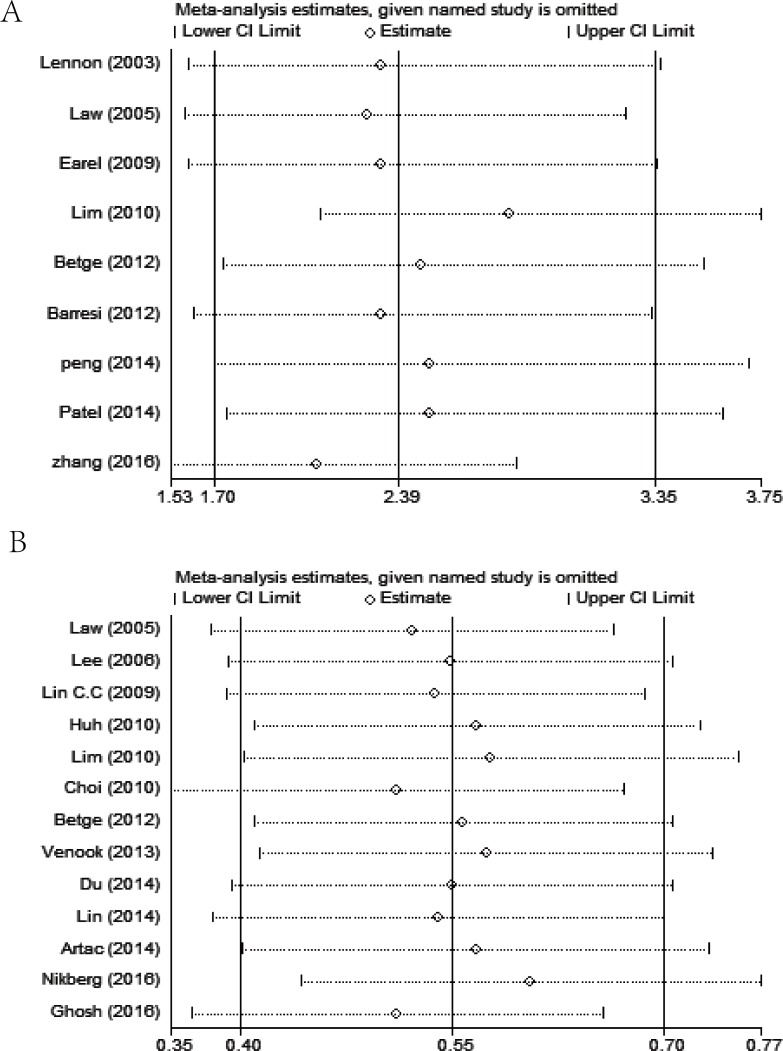
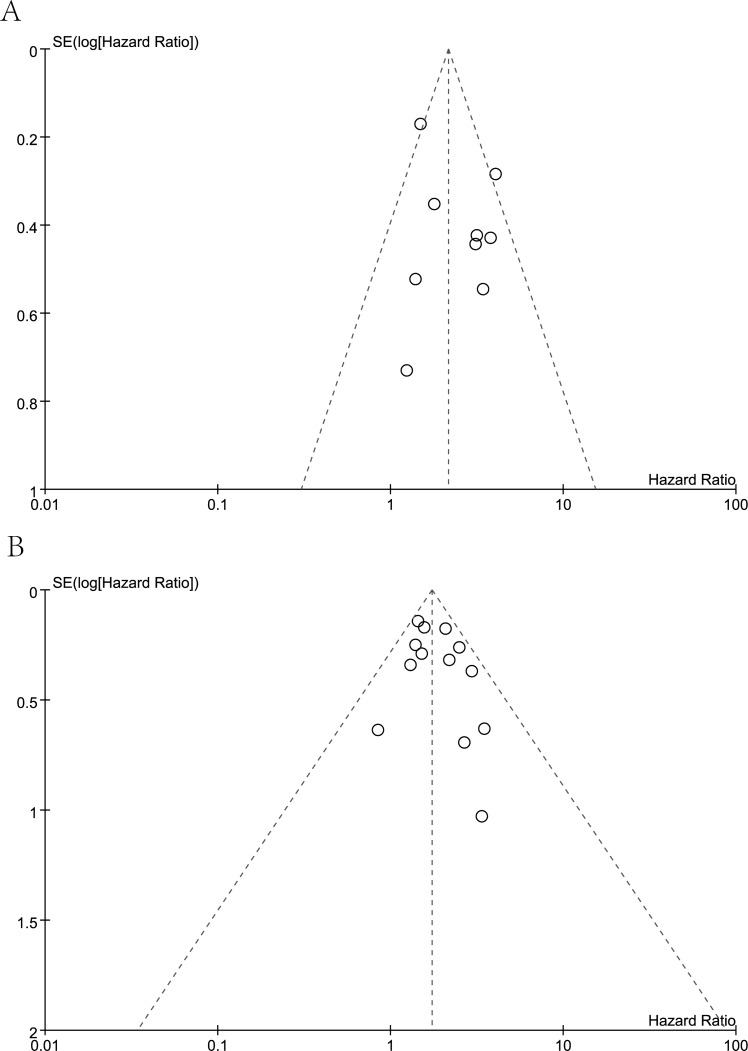
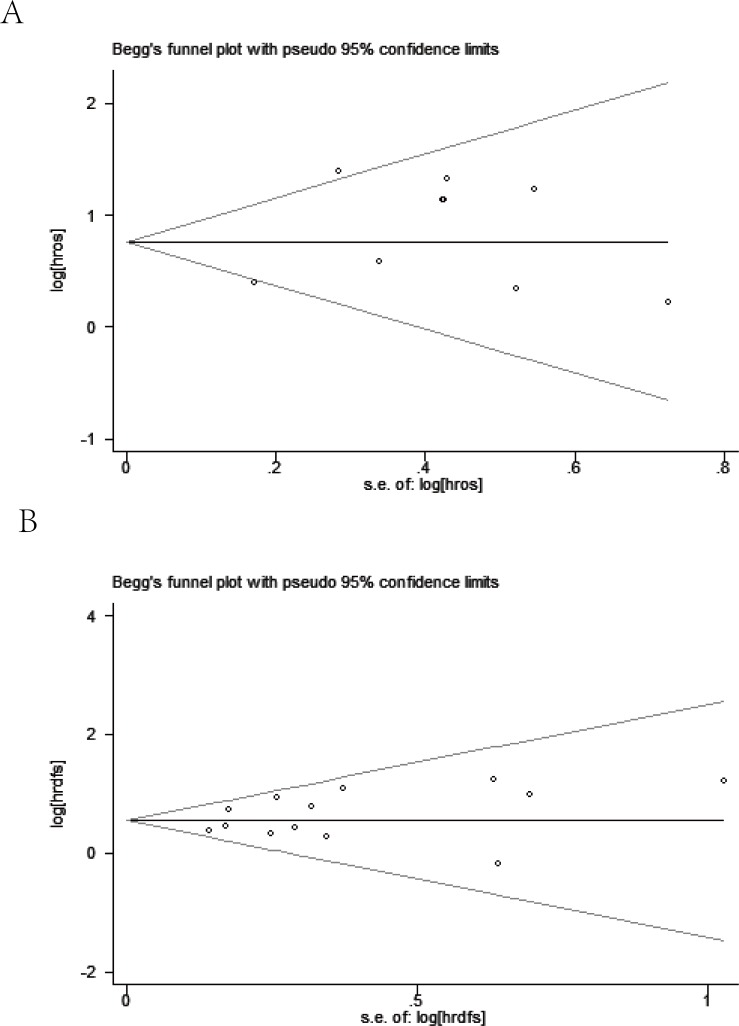
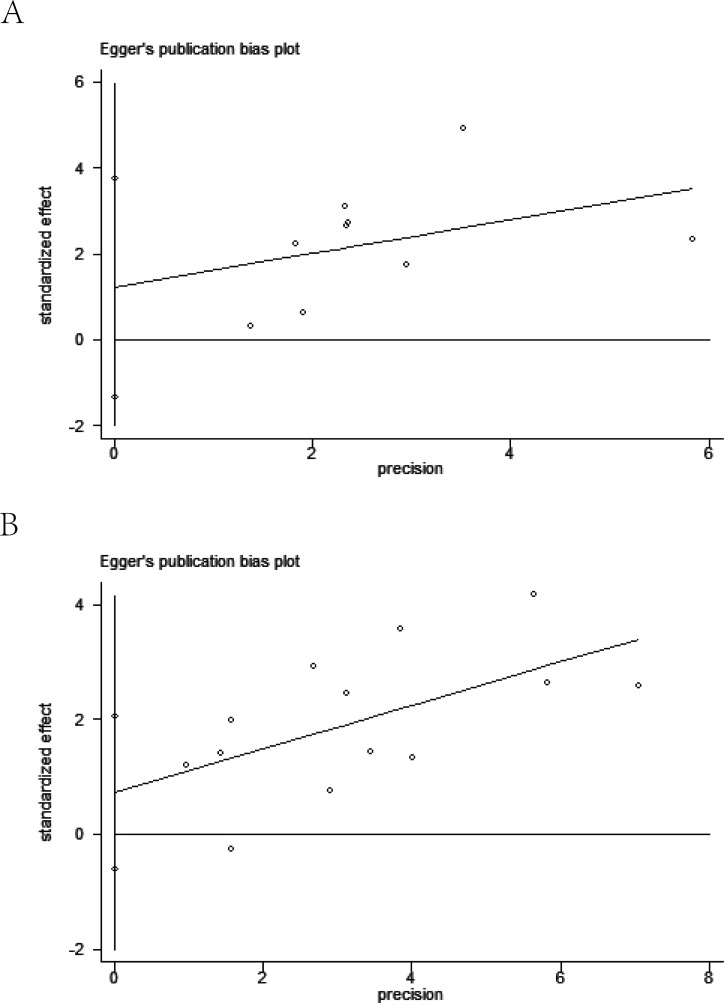
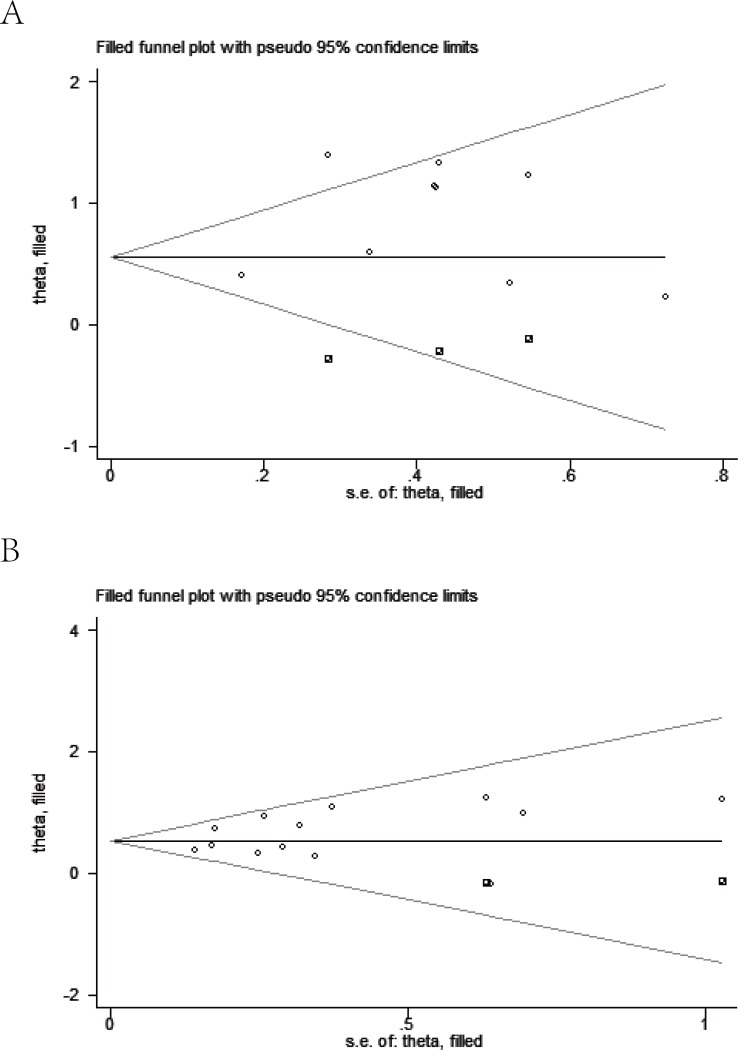
The prognostic value of lymphovascular invasion (LVI) in stage I/II colorectal cancer (CRC) does not reach a consensus. To systematically assess prognostic significance of LVI, databases of PubMed, Web of Science, and Embase were searched from inception up to 10 Dec 2016. The pooled hazard ratio (HR) and 95% confidence intervals (CI) were used to determine the prognostic effects. Nineteen relevant studies including 9881 total patients were enrolled. Our results showed that LVI is significantly associated with poor prognosis in overall survival (OS) (HR=2.15, 95 % CI=1.72-2.68, P < 0.01) and disease-free survival (DFS) (HR=1.73, 95% CI=1.50-1.99, P < 0.01), which is similar in stage II patients. Further subgroup analysis revealed that the significance of the association between LVI and worse prognosis in CRC patients is not affected by below factors, including geographic setting, LVI positive rate, treatment, tumor site, and quality of the study. The current meta-analysis suggests that LVI may be a poor prognostic factor for stage I/II CRC patients.
Keywords: colorectal cancer; lymphovascular invasion; meta-analysis; stage I/II; survival.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
-
Prognostic and clinicopathological significance of circulating tumor cells detected by RT-PCR in non-metastatic colorectal cancer: a meta-analysis and systematic review.BMC Cancer. 2017 Nov 7;17(1):725. doi: 10.1186/s12885-017-3704-8. BMC Cancer. 2017. PMID: 29115932 Free PMC article.
-
Lymphovascular invasion as a prognostic indicator in stage I non-small cell lung cancer: a systematic review and meta-analysis.Ann Thorac Surg. 2014 Mar;97(3):965-71. doi: 10.1016/j.athoracsur.2013.11.002. Epub 2014 Jan 11. Ann Thorac Surg. 2014. PMID: 24424014
-
Increased platelet-lymphocyte ratio closely relates to inferior clinical features and worse long-term survival in both resected and metastatic colorectal cancer: an updated systematic review and meta-analysis of 24 studies.Oncotarget. 2017 May 9;8(19):32356-32369. doi: 10.18632/oncotarget.16020. Oncotarget. 2017. PMID: 28404961 Free PMC article.
-
The impact of lymphovascular invasion in patients treated with radical nephroureterectomy for upper tract urothelial carcinoma: An extensive updated systematic review and meta-analysis.Urol Oncol. 2022 Jun;40(6):243-261. doi: 10.1016/j.urolonc.2022.01.014. Epub 2022 Feb 28. Urol Oncol. 2022. PMID: 35241364
Cited by
-
Lymphovascular invasion in colorectal cancers: can we predict it preoperatively?Ann Coloproctol. 2024 Jun;40(3):245-252. doi: 10.3393/ac.2023.00458.0065. Epub 2024 Jun 25. Ann Coloproctol. 2024. PMID: 38946095 Free PMC article.
-
Lymphovascular invasion, perineural invasion, and tumor budding are prognostic factors for stage I colon cancer recurrence.Int J Colorectal Dis. 2020 May;35(5):881-885. doi: 10.1007/s00384-020-03548-4. Epub 2020 Feb 28. Int J Colorectal Dis. 2020. PMID: 32112198
-
KCNQ1 and lymphovascular invasion are key features in a prognostic classifier for stage II and III colon cancer.BMC Cancer. 2022 Apr 8;22(1):372. doi: 10.1186/s12885-022-09473-9. BMC Cancer. 2022. PMID: 35395779 Free PMC article.
-
Characteristics and outcomes of rectal cancer in patients with inflammatory bowel disease: a single-center experience.Updates Surg. 2024 Jan;76(1):119-126. doi: 10.1007/s13304-023-01660-y. Epub 2023 Oct 9. Updates Surg. 2024. PMID: 37814150
-
Chronic Obstructive Pulmonary Disease and Its Acute Exacerbation before Colon Adenocarcinoma Treatment Are Associated with Higher Mortality: A Propensity Score-Matched, Nationwide, Population-Based Cohort Study.Cancers (Basel). 2021 Sep 21;13(18):4728. doi: 10.3390/cancers13184728. Cancers (Basel). 2021. PMID: 34572955 Free PMC article.
References
-
- Zlobec I, Lugli A. Prognostic and predictive factors in colorectal cancer. J Clin Pathol. 2008;61:561–569. - PubMed
-
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) in Colon Cancer (Version 1.2017) 2017 Available at: http://wwwnccnorg/professionals/physician_gls/f_guidelinesasp.
-
- Talbot IC, Ritchie S, Leighton MH, Hughes AO, Bussey HJ, Morson BC. The clinical significance of invasion of veins by rectal cancer. The British journal of surgery. 1980;67:439–442. - PubMed
-
- Horn A, Dahl O, Morild I. The role of venous and neural invasion on survival in rectal adenocarcinoma. Dis Colon Rectum. 1990;33:598–601. - PubMed
-
- Chapuis PH, Dent OF, Fisher R, Newland RC, Pheils MT, Smyth E, Colquhoun K. A multivariate analysis of clinical and pathological variables in prognosis after resection of large bowel cancer. The British journal of surgery. 1985;72:698–702. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
