

Effects of Antiretroviral Therapy and Depressive Symptoms on All-Cause Mortality Among HIV-Infected Women
- PMID: 28430844
- PMCID: PMC5430940
- DOI: 10.1093/aje/kww192
Effects of Antiretroviral Therapy and Depressive Symptoms on All-Cause Mortality Among HIV-Infected Women
Abstract
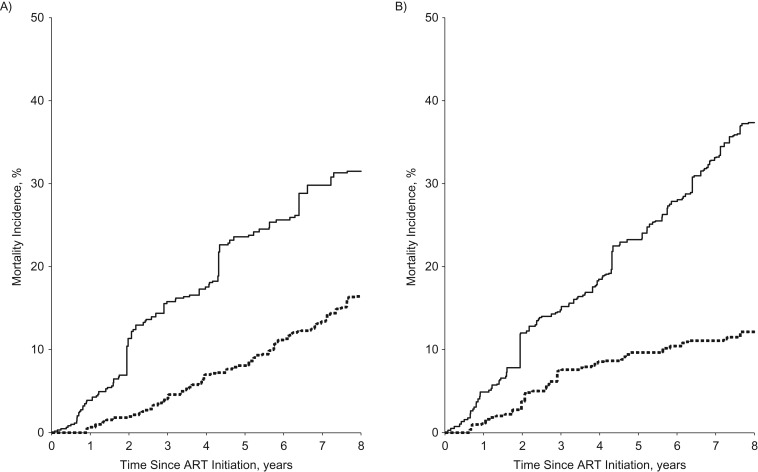
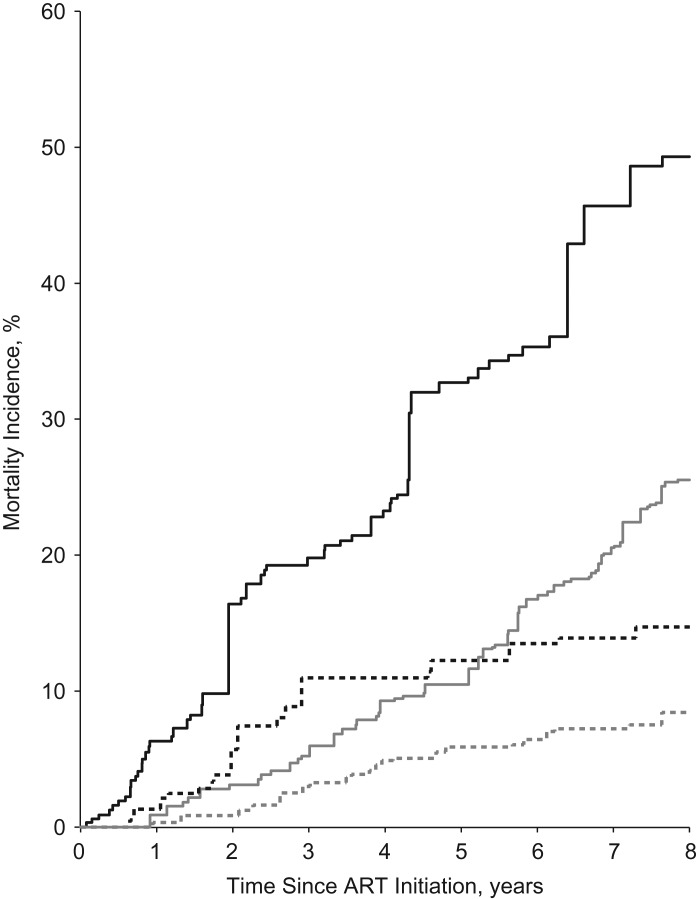
Depression affects up to 30% of human immunodeficiency virus (HIV)-infected individuals. We estimated joint effects of antiretroviral therapy (ART) initiation and depressive symptoms on time to death using a joint marginal structural model and data from a cohort of HIV-infected women from the Women's Interagency HIV Study (conducted in the United States) from 1998-2011. Among 848 women contributing 6,721 years of follow-up, 194 participants died during follow-up, resulting in a crude mortality rate of 2.9 per 100 women-years. Cumulative mortality curves indicated greatest mortality for women who reported depressive symptoms and had not initiated ART. The hazard ratio for depressive symptoms was 3.38 (95% confidence interval (CI): 2.15, 5.33) and for ART was 0.47 (95% CI: 0.31, 0.70). Using a reference category of women without depressive symptoms who had initiated ART, the hazard ratio for women with depressive symptoms who had initiated ART was 3.60 (95% CI: 2.02, 6.43). For women without depressive symptoms who had not started ART, the hazard ratio was 2.36 (95% CI: 1.16, 4.81). Among women reporting depressive symptoms who had not started ART, the hazard ratio was 7.47 (95% CI: 3.91, 14.3). We found a protective effect of ART initiation on mortality, as well as a harmful effect of depressive symptoms, in a cohort of HIV-infected women.
Keywords: HIV; antiretroviral therapy; cohort studies; depression; marginal structural models; mortality; proportional hazards models; women.
© The Author 2017. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Mortality under plausible interventions on antiretroviral treatment and depression in HIV-infected women: an application of the parametric g-formula.Ann Epidemiol. 2017 Dec;27(12):783-789.e2. doi: 10.1016/j.annepidem.2017.08.021. Epub 2017 Sep 5. Ann Epidemiol. 2017. PMID: 28939001 Free PMC article.
-
Factors associated with attrition, mortality, and loss to follow up after antiretroviral therapy initiation: data from an HIV cohort study in India.Glob Health Action. 2013 Sep 12;6:21682. doi: 10.3402/gha.v6i0.21682. Glob Health Action. 2013. PMID: 24028937 Free PMC article.
-
Association between Use of Methadone, Other Central Nervous System Depressants, and QTc Interval-Prolonging Medications and Risk of Mortality in a Large Cohort of Women Living with or at Risk for Human Immunodeficiency Virus Infection.Pharmacotherapy. 2019 Sep;39(9):899-911. doi: 10.1002/phar.2312. Epub 2019 Aug 13. Pharmacotherapy. 2019. PMID: 31332819 Free PMC article.
-
Treatment response and mortality among patients starting antiretroviral therapy with and without Kaposi sarcoma: a cohort study.PLoS One. 2013 Jun 5;8(6):e64392. doi: 10.1371/journal.pone.0064392. Print 2013. PLoS One. 2013. PMID: 23755122 Free PMC article.
-
Survival benefit of initiating antiretroviral therapy in HIV-infected persons in different CD4+ cell strata.Ann Intern Med. 2003 Apr 15;138(8):620-6. doi: 10.7326/0003-4819-138-8-200304150-00007. Ann Intern Med. 2003. PMID: 12693883
Cited by
-
HIV Infection and Related Mental Disorders.Brain Sci. 2021 Feb 17;11(2):248. doi: 10.3390/brainsci11020248. Brain Sci. 2021. PMID: 33671125 Free PMC article. Review.
-
Lessons Learned from a Community-led, Pilot Teletherapy Group for Older Women Living with Depression and HIV.AIDS Behav. 2024 Dec;28(12):4079-4093. doi: 10.1007/s10461-024-04468-y. Epub 2024 Sep 2. AIDS Behav. 2024. PMID: 39222185 Free PMC article.
-
Psychological distress in women and men living with HIV in Spain: a cross-sectional telephone survey.Evid Based Ment Health. 2020 Aug;23(3):91-99. doi: 10.1136/ebmental-2019-300138. Epub 2020 Jul 14. Evid Based Ment Health. 2020. PMID: 32665249 Free PMC article.
-
Mental health and HIV/AIDS: the need for an integrated response.AIDS. 2019 Jul 15;33(9):1411-1420. doi: 10.1097/QAD.0000000000002227. AIDS. 2019. PMID: 30950883 Free PMC article. Review.
-
Measurement of depression treatment among patients receiving HIV primary care: Whither the truth?J Affect Disord. 2018 Apr 1;230:50-55. doi: 10.1016/j.jad.2017.12.068. Epub 2018 Jan 3. J Affect Disord. 2018. PMID: 29407538 Free PMC article.
References
-
- Bing EG, Burnam MA, Longshore D, et al. . Psychiatric disorders and drug use among human immunodeficiency virus-infected adults in the United States. Arch Gen Psychiatry. 2001;58(8):721–728. - PubMed
-
- Pence BW, Miller WC, Whetten K, et al. . Prevalence of DSM-IV-defined mood, anxiety, and substance use disorders in an HIV clinic in the Southeastern United States. J Acquir Immune Defic Syndr. 2006;42(3):298–306. - PubMed
-
- Israelski DM, Prentiss DE, Lubega S, et al. . Psychiatric co-morbidity in vulnerable populations receiving primary care for HIV/AIDS. AIDS Care. 2007;19(2):220–225. - PubMed
-
- Ciesla JA, Roberts JE. Meta-analysis of the relationship between HIV infection and risk for depressive disorders. Am J Psychiatry. 2001;158(5):725–730. - PubMed
MeSH terms
Substances
Grants and funding
- U01 AI103397/AI/NIAID NIH HHS/United States
- U01 AI031834/AI/NIAID NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- U01 AI103401/AI/NIAID NIH HHS/United States
- U01 AI103408/AI/NIAID NIH HHS/United States
- U01 HL146194/HL/NHLBI NIH HHS/United States
- U01 AI103390/AI/NIAID NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- R01 AI100654/AI/NIAID NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
