

Prediction of sudden and non-sudden cardiac death in post-infarction patients with reduced left ventricular ejection fraction by periodic repolarization dynamics: MADIT-II substudy
- PMID: 28431133
- PMCID: PMC5837472
- DOI: 10.1093/eurheartj/ehx161
Prediction of sudden and non-sudden cardiac death in post-infarction patients with reduced left ventricular ejection fraction by periodic repolarization dynamics: MADIT-II substudy
Abstract
Aims: To test the value of Periodic Repolarization Dynamics (PRD), a recently validated electrocardiographic marker of sympathetic activity, as a novel approach to predict sudden cardiac death (SCD) and non-sudden cardiac death (N-SCD) and to improve identification of patients that profit from ICD-implantation.
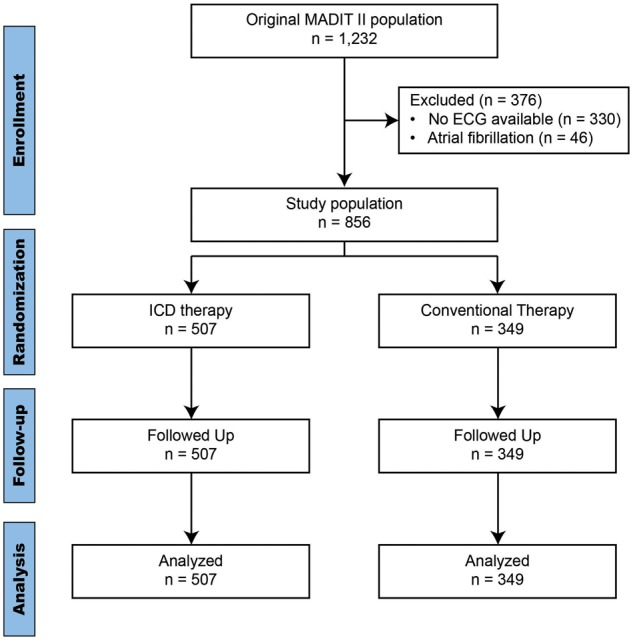
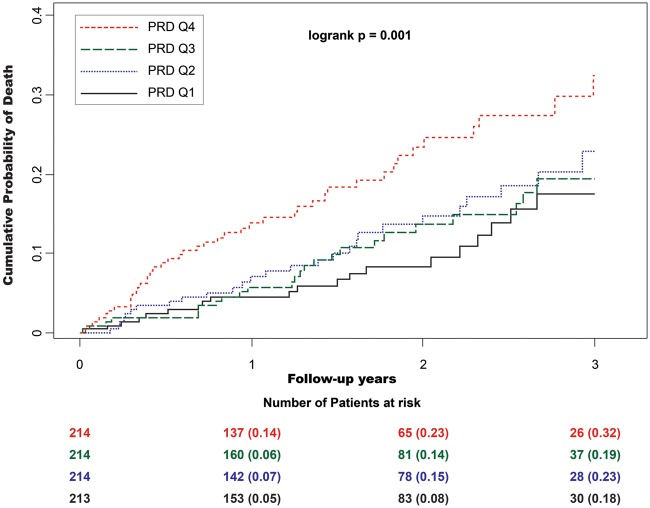
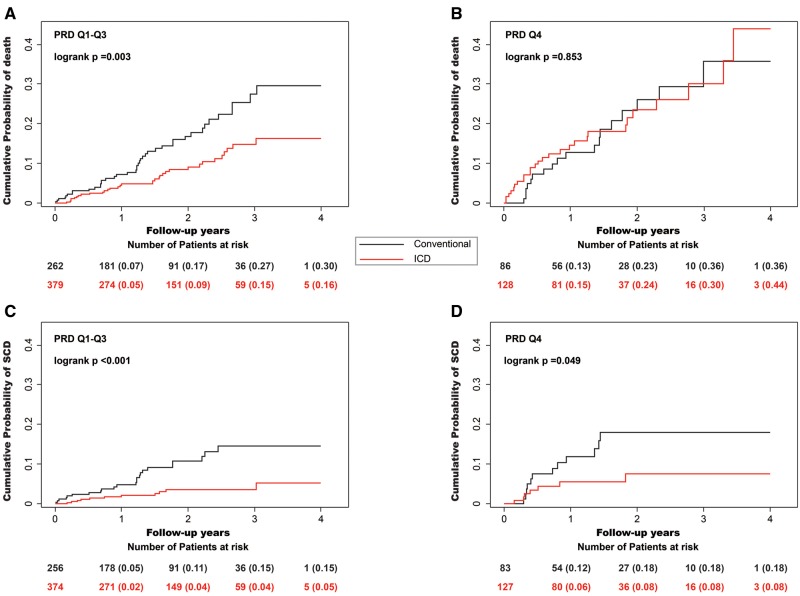
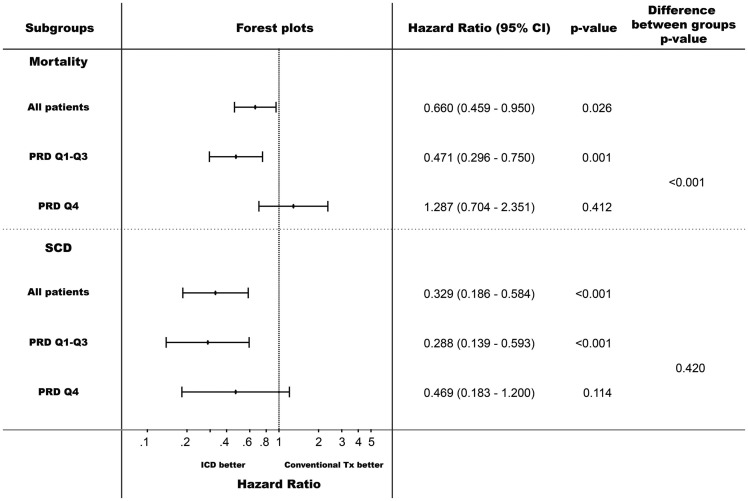
Methods and results: We included 856 post-infarction patients with left-ventricular ejection fraction (LVEF) ≤30% of the MADIT-II trial in sinus rhythm. Of these, 507 and 348 patients were randomized to ICD or conventional treatment. PRD was assessed from multipolar 10-min baseline ECGs. Primary and secondary endpoints were total mortality, SCD and N-SCD. Multivariable analyses included treatment group, QRS-duration, New York Heart Association classification, blood-urea nitrogen, diabetes mellitus, beta-blocker therapy and LVEF. During follow-up of 20.4 months, 119 patients died (53 SCD and 36 N-SCD). On multivariable analyses, increased PRD was a significant predictor of mortality (standardized coefficient 1.37[1.19-1.59]; P < 0.001) and SCD (1.40 [1.13-1.75]; P = 0.003) but also predicted N-SCD (1.41[1.10-1.81]; P = 0.006). While increased PRD predicted SCD in conventionally treated patients (1.61[1.23-2.11]; P < 0.001), it was predictive of N-SCD (1.63[1.28-2.09]; P < 0.001) and adequate ICD-therapies (1.20[1.03-1.39]; P = 0.017) in ICD-treated patients. ICD-treatment substantially reduced mortality in the lowest three PRD-quartiles by 53% (P = 0.001). However, there was no effect in the highest PRD-quartile (mortality increase by 29%; P = 0.412; P < 0.001 for difference) as the reduction of SCD was compensated by an increase of N-SCD.
Conclusion: In post-infarction patients with impaired LVEF, PRD is a significant predictor of SCD and N-SCD. Assessment of PRD is a promising tool to identify post-MI patients with reduced LVEF who might benefit from intensified treatment.
Keywords: Electrocardiography; Implantable cardioverter defibrillator; Risk prediction; Sudden cardiac death; Sympathetic nervous system.
© The Author 2017. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Cardiac electrophysiology: signals to decrypt and to decipher.Eur Heart J. 2017 Jul 14;38(27):2119-2121. doi: 10.1093/eurheartj/ehx212. Eur Heart J. 2017. PMID: 28472261 No abstract available.
Similar articles
-
ECG quantification of myocardial scar and risk stratification in MADIT-II.Ann Noninvasive Electrocardiol. 2013 Sep;18(5):427-35. doi: 10.1111/anec.12065. Epub 2013 Jun 9. Ann Noninvasive Electrocardiol. 2013. PMID: 24047486 Free PMC article. Clinical Trial.
-
Implantable cardioverter defibrillators. Prophylactic use: an evidence-based analysis.Ont Health Technol Assess Ser. 2005;5(14):1-74. Epub 2005 Sep 1. Ont Health Technol Assess Ser. 2005. PMID: 23074465 Free PMC article.
-
Risk stratification after myocardial infarction: is left ventricular ejection fraction enough to prevent sudden cardiac death?Eur Heart J. 2013 Jul;34(26):1964-71. doi: 10.1093/eurheartj/eht109. Epub 2013 May 3. Eur Heart J. 2013. PMID: 23644180 Review.
-
Periodic Repolarization Dynamics Identifies ICD Responders in Nonischemic Cardiomyopathy: A DANISH Substudy.Circulation. 2022 Mar 8;145(10):754-764. doi: 10.1161/CIRCULATIONAHA.121.056464. Epub 2021 Dec 10. Circulation. 2022. PMID: 34889650 Clinical Trial.
-
Effect of left ventricular ejection fraction and QRS duration on the survival benefit of implantable cardioverter-defibrillators: meta-analysis of primary prevention trials.Heart Rhythm. 2013 Feb;10(2):200-6. doi: 10.1016/j.hrthm.2012.10.039. Epub 2012 Oct 27. Heart Rhythm. 2013. PMID: 23107652 Review.
Cited by
-
Rationale and design of the EU-CERT-ICD prospective study: comparative effectiveness of prophylactic ICD implantation.ESC Heart Fail. 2019 Feb;6(1):182-193. doi: 10.1002/ehf2.12367. Epub 2018 Oct 9. ESC Heart Fail. 2019. PMID: 30299600 Free PMC article.
-
Estimation of anaerobic threshold by cardiac repolarization instability: a prospective validation study.BMC Sports Sci Med Rehabil. 2021 Aug 6;13(1):85. doi: 10.1186/s13102-021-00312-1. BMC Sports Sci Med Rehabil. 2021. PMID: 34362449 Free PMC article.
-
Renal resistive index and long-term outcome in patients with coronary artery disease.BMC Cardiovasc Disord. 2020 Jul 6;20(1):322. doi: 10.1186/s12872-020-01607-w. BMC Cardiovasc Disord. 2020. PMID: 32631235 Free PMC article.
-
Complex Interaction Between Low-Frequency APD Oscillations and Beat-to-Beat APD Variability in Humans Is Governed by the Sympathetic Nervous System.Front Physiol. 2020 Jan 22;10:1582. doi: 10.3389/fphys.2019.01582. eCollection 2019. Front Physiol. 2020. PMID: 32038279 Free PMC article.
-
QRS complex and T wave planarity for the efficacy prediction of automatic implantable defibrillators.Heart. 2024 Jan 10;110(3):178-187. doi: 10.1136/heartjnl-2023-322878. Heart. 2024. PMID: 37714697 Free PMC article.
References
-
- Epstein AE, DiMarco JP, Ellenbogen KA, Estes NAM, Freedman RA, Gettes LS, Gillinov AM, Gregoratos G, Hammill SC, Hayes DL, Hlatky MA, Newby LK, Page RL, Schoenfeld MH, Silka MJ, Stevenson LW, Sweeney MO; American College of Cardiology Foundation, American Heart Association Task Force on Practice Guidelines, Heart Rhythm Society. 2012 ACCF/AHA/HRS focused update incorporated into the ACCF/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation 2013;127;e283–e352. - PubMed
-
- Priori SG, Blömstrom-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck KH, Hernández-Madrid A, Nikolaou N, Norekvål TM, Spaulding C, van Veldhuisen DJ; Authors/Task Force Members, Document Reviewers. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J 2015;36:2793–2867. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML; Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med 2002;346:877–883. - PubMed
-
- Moss AJ, Greenberg H, Case RB, Zareba W, Hall WJ, Brown MW, Daubert JP, McNitt S, Andrews ML, Elkin AD; Multicenter Automatic Defibrillator Implantation Trial-II (MADIT-II) Research Group. Long-term clinical course of patients after termination of ventricular tachyarrhythmia by an implanted defibrillator. Circulation 2004;110:3760–3765. - PubMed
-
- Triposkiadis F, Karayannis G, Giamouzis G, Skoularigis J, Louridas G, Butler J.. The sympathetic nervous system in heart failure physiology, pathophysiology, and clinical implications. J Am Coll Cardiol 2009;54:1747–1762. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
