

Monitoring quality and coverage of harm reduction services for people who use drugs: a consensus study
- PMID: 28431584
- PMCID: PMC5401609
- DOI: 10.1186/s12954-017-0141-6
Monitoring quality and coverage of harm reduction services for people who use drugs: a consensus study
Abstract
Background and aims: Despite advances in our knowledge of effective services for people who use drugs over the last decades globally, coverage remains poor in most countries, while quality is often unknown. This paper aims to discuss the historical development of successful epidemiological indicators and to present a framework for extending them with additional indicators of coverage and quality of harm reduction services, for monitoring and evaluation at international, national or subnational levels. The ultimate aim is to improve these services in order to reduce health and social problems among people who use drugs, such as human immunodeficiency virus (HIV) and hepatitis C virus (HCV) infection, crime and legal problems, overdose (death) and other morbidity and mortality.
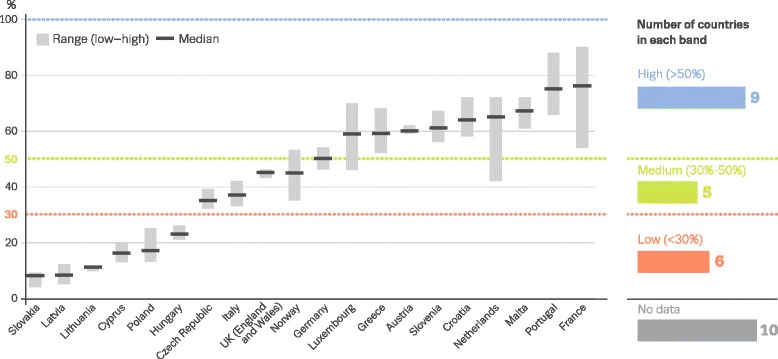
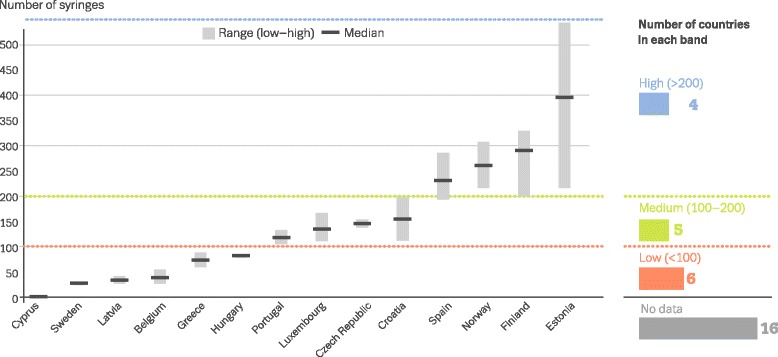
Methods and results: The framework was developed collaboratively using consensus methods involving nominal group meetings, review of existing quality standards, repeated email commenting rounds and qualitative analysis of opinions/experiences from a broad range of professionals/experts, including members of civil society and organisations representing people who use drugs. Twelve priority candidate indicators are proposed for opioid agonist therapy (OAT), needle and syringe programmes (NSP) and generic cross-cutting aspects of harm reduction (and potentially other drug) services. Under the specific OAT indicators, priority indicators included 'coverage', 'waiting list time', 'dosage' and 'availability in prisons'. For the specific NSP indicators, the priority indicators included 'coverage', 'number of needles/syringes distributed/collected', 'provision of other drug use paraphernalia' and 'availability in prisons'. Among the generic or cross-cutting indicators the priority indicators were 'infectious diseases counselling and care', 'take away naloxone', 'information on safe use/sex' and 'condoms'. We discuss conditions for the successful development of the suggested indicators and constraints (e.g. funding, ideology). We propose conducting a pilot study to test the feasibility and applicability of the proposed indicators before their scaling up and routine implementation, to evaluate their effectiveness in comparing service coverage and quality across countries.
Conclusions: The establishment of an improved set of validated and internationally agreed upon best practice indicators for monitoring harm reduction service will provide a structural basis for public health and epidemiological studies and support evidence and human rights-based health policies, services and interventions.
Keywords: Best practice; Coverage; Drug services; Epidemiology; Evidence-based; HCV; HIV; Harm reduction; Indicators; Injecting drug users/IDU; Interventions; Knowledge exchange; Monitoring; People who inject drugs/PWID; People who use drugs/PWUD; Substance abuse.
Figures
References
-
- Harm Reduction International. The global state of harm reduction 2016. Edited by Stone K. London: Harm Reduction International; 2016. https://www.hri.global/files/2016/11/14/GSHR2016_14nov.pdf. Accessed 20 Mar 2017.
-
- Committee on the Prevention of HIV Infection among Injecting Drug Users in High-Risk Countries. Preventing HIV infection among injecting drug users in high risk countries: an assessment of the evidence. Washington: Institute of Medicine of the National Academies; 2006.
-
- WHO. Evidence for action series—technical papers and policy briefs on HIV/AIDS and injecting drug users. Geneva: WHO; 2015. http://www.who.int/hiv/pub/idu/evidence_for_action/en/. Accessed 20 Mar 2017.
-
- ECDC, EMCDDA. Prevention and control of infectious diseases among people who inject drugs. Stockholm: ECDC/EMCDDA; 2011. https://goo.gl/2rQBzv. Accessed 20 Mar 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
