

Systolic Blood Pressure Trajectory, Frailty, and All-Cause Mortality >80 Years of Age: Cohort Study Using Electronic Health Records
- PMID: 28432148
- PMCID: PMC5472195
- DOI: 10.1161/CIRCULATIONAHA.116.026687
Systolic Blood Pressure Trajectory, Frailty, and All-Cause Mortality >80 Years of Age: Cohort Study Using Electronic Health Records
Abstract
Background: Clinical trials show benefit from lowering systolic blood pressure (SBP) in people ≥80 years of age, but nonrandomized epidemiological studies suggest lower SBP may be associated with higher mortality. This study aimed to evaluate associations of SBP with all-cause mortality by frailty category >80 years of age and to evaluate SBP trajectories before death.
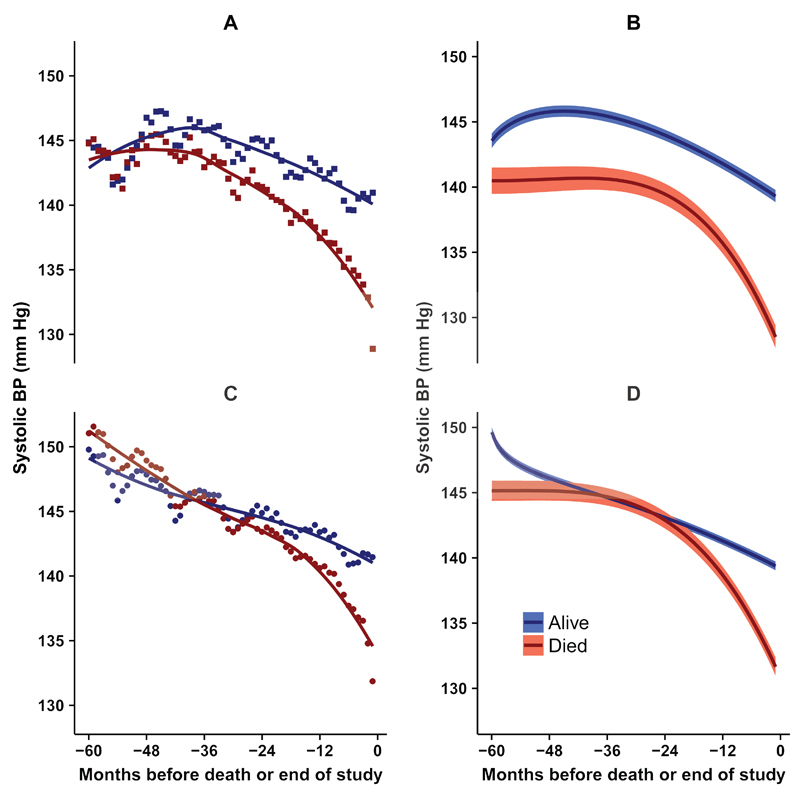
Methods: A population-based cohort study was conducted using electronic health records of 144 403 participants ≥80 years of age registered with family practices in the United Kingdom from 2001 to 2014. Participants were followed for ≤5 years. Clinical records of SBP were analyzed. Frailty status was classified using the e-Frailty Index into the categories of fit, mild, moderate, and severe. All-cause mortality was evaluated by frailty status and mean SBP in Cox proportional-hazards models. SBP trajectories were evaluated using person months as observations, with mean SBP and antihypertensive treatment status estimated for each person month. Fractional polynomial models were used to estimate SBP trajectories over 5 years before death.
Results: During follow-up, 51 808 deaths occurred. Mortality rates increased with frailty level and were greatest at SBP <110 mm Hg. In fit women, mortality was 7.7 per 100 person years at SBP 120 to 139 mm Hg, 15.2 at SBP 110 to 119 mm Hg, and 22.7 at SBP <110 mm Hg. For women with severe frailty, rates were 16.8, 25.2, and 39.6, respectively. SBP trajectories showed an accelerated decline in the last 2 years of life. The relative odds of SBP <120 mm Hg were higher in the last 3 months of life than 5 years previously in both treated (odds ratio, 6.06; 95% confidence interval, 5.40-6.81) and untreated (odds ratio, 6.31; 95% confidence interval, 5.30-7.52) patients. There was no evidence of intensification of antihypertensive therapy in the final 2 years of life.
Conclusions: A terminal decline of SBP in the final 2 years of life suggests that nonrandomized epidemiological associations of low SBP with higher mortality may be accounted for by reverse causation if participants with lower blood pressure values are closer, on average, to the end of life.
Keywords: antihypertensive treatment; elderly; frailty; hypertension; mortality; primary care.
© 2017 The Authors.
Figures
Comment in
-
Reverse Causality in Cardiovascular Epidemiological Research: More Common Than Imagined?Circulation. 2017 Jun 13;135(24):2369-2372. doi: 10.1161/CIRCULATIONAHA.117.028307. Circulation. 2017. PMID: 28606949 No abstract available.
Similar articles
-
Systolic Blood Pressure and Mortality in Community-Dwelling Older Adults: Frailty as an Effect Modifier.Hypertension. 2022 Jan;79(1):24-32. doi: 10.1161/HYPERTENSIONAHA.121.17530. Epub 2021 Oct 25. Hypertension. 2022. PMID: 34689594
-
Association between trajectories of systolic blood pressure and frailty outcome in middle-aged and older adults.J Nutr Health Aging. 2024 May;28(5):100202. doi: 10.1016/j.jnha.2024.100202. Epub 2024 Mar 8. J Nutr Health Aging. 2024. PMID: 38460319
-
Blood pressure in frail older adults: associations with cardiovascular outcomes and all-cause mortality.Age Ageing. 2020 Aug 24;49(5):807-813. doi: 10.1093/ageing/afaa028. Age Ageing. 2020. PMID: 32133525 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Blood pressure targets in adults with hypertension.Cochrane Database Syst Rev. 2020 Dec 17;12(12):CD004349. doi: 10.1002/14651858.CD004349.pub3. Cochrane Database Syst Rev. 2020. PMID: 33332584 Free PMC article.
Cited by
-
Blood pressure in the longevous population with different status of hypertension and frailty.Hypertens Res. 2024 Apr;47(4):959-969. doi: 10.1038/s41440-023-01499-1. Epub 2023 Nov 20. Hypertens Res. 2024. PMID: 37985739
-
Impact of Frailty on the Relationship between Blood Pressure and Cardiovascular Diseases and Mortality in Young-Old Adults.J Pers Med. 2022 Mar 8;12(3):418. doi: 10.3390/jpm12030418. J Pers Med. 2022. PMID: 35330418 Free PMC article.
-
Identifying Frail Patients by Using Electronic Health Records in Primary Care: Current Status and Future Directions.Front Public Health. 2022 Jun 22;10:901068. doi: 10.3389/fpubh.2022.901068. eCollection 2022. Front Public Health. 2022. PMID: 35812471 Free PMC article. Review.
-
Changes in late-life systolic blood pressure and all-cause mortality among oldest-old people in China: the chinese longitudinal healthy longevity survey.BMC Geriatr. 2021 Oct 18;21(1):562. doi: 10.1186/s12877-021-02492-4. BMC Geriatr. 2021. PMID: 34663235 Free PMC article.
-
Relationship between changes in late-life blood pressure and the risk of frailty and mortality among older population in China: a cohort study based on CLHLS.Hypertens Res. 2024 Jul;47(7):1881-1891. doi: 10.1038/s41440-024-01674-y. Epub 2024 Apr 10. Hypertens Res. 2024. PMID: 38600277
References
-
- Safar ME, Levy BI, Struijker-Boudier H. Current perspectives on arterial stiffness and pulse pressure in hypertension and cardiovascular diseases. Circulation. 2003;107:2864–2869. - PubMed
-
- Staessen JA, Gasowski J, Wang JG, Thijs L, Hond ED, Boissel J-P, Coope J, Ekbom T, Gueyffier F, Liu L, Kerlikowske K, et al. Risks of untreated and treated isolated systolic hypertension in the elderly: meta-analysis of outcome trials. Lancet. 2000;355:865–872. - PubMed
-
- Liu L, Wang JG, Gong L, Liu G, Staessen JA. Comparison of active treatment and placebo in older Chinese patients with isolated systolic hypertension. Systolic Hypertension in China (Syst-China) Collaborative Group. J Hypertension. 1998;16:1823–1829. - PubMed
-
- Staessen JA, Fagard R, Thijs L, Celis H, Arabidze GG, Birkenhager WH, Bulpitt CJ, de Leeuw PW, Dollery CT, Fletcher AE. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet. 1997;350:757–764. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
