

A prospective, observational cohort study of the seasonal dynamics of airway pathogens in the aetiology of exacerbations in COPD
- PMID: 28432209
- PMCID: PMC5738531
- DOI: 10.1136/thoraxjnl-2016-209023
A prospective, observational cohort study of the seasonal dynamics of airway pathogens in the aetiology of exacerbations in COPD
Abstract
Background: The aetiology of acute exacerbations of COPD (AECOPD) is incompletely understood. Understanding the relationship between chronic bacterial airway infection and viral exposure may explain the incidence and seasonality of these events.
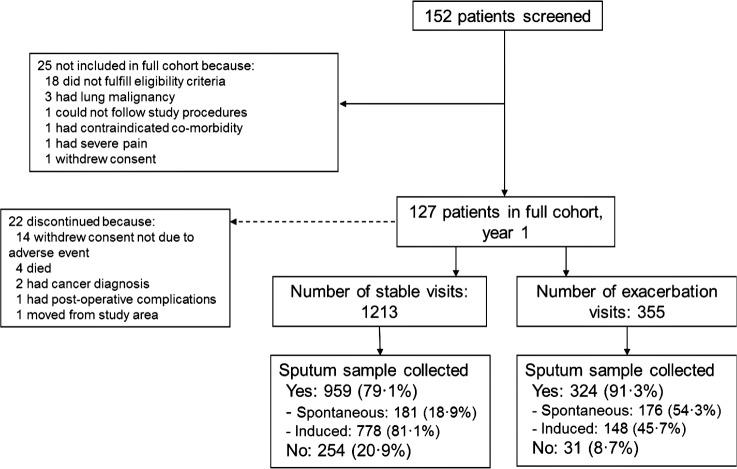
Methods: In this prospective, observational cohort study (NCT01360398), patients with COPD aged 40-85 years underwent sputum sampling monthly and at exacerbation for detection of bacteria and viruses. Results are presented for subjects in the full cohort, followed for 1 year. Interactions between exacerbation occurrence and pathogens were investigated by generalised estimating equation and stratified conditional logistic regression analyses.
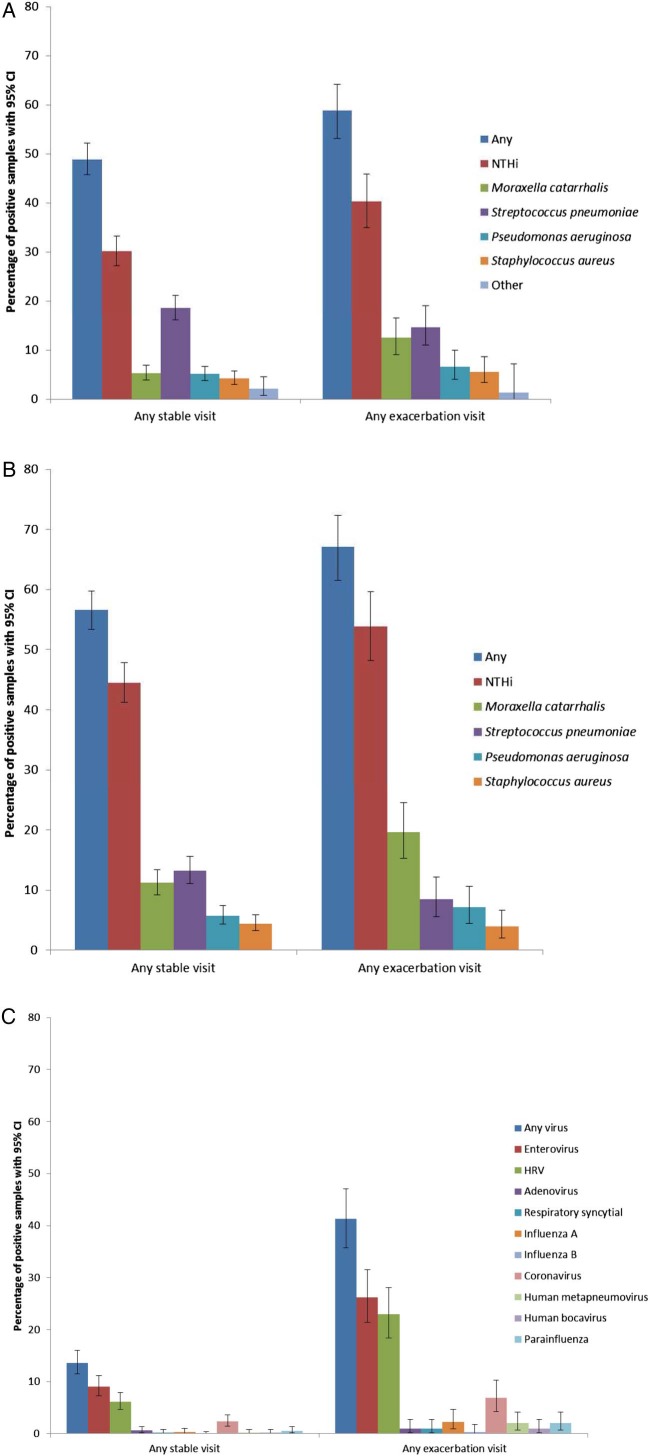
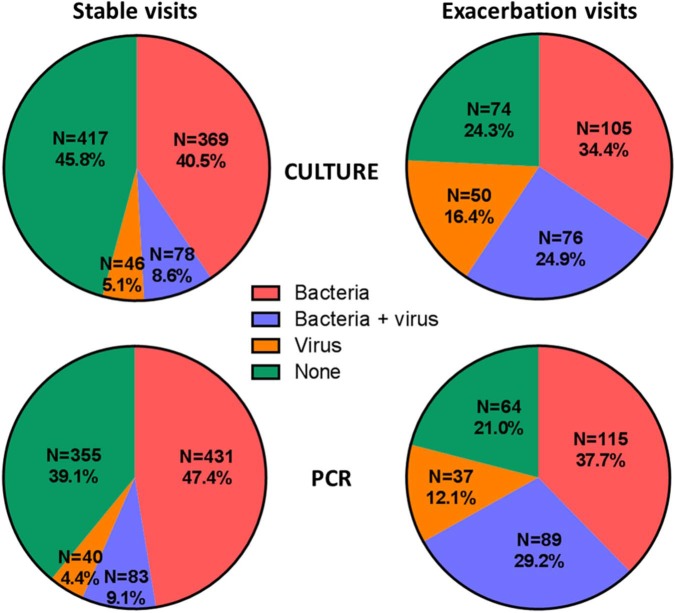
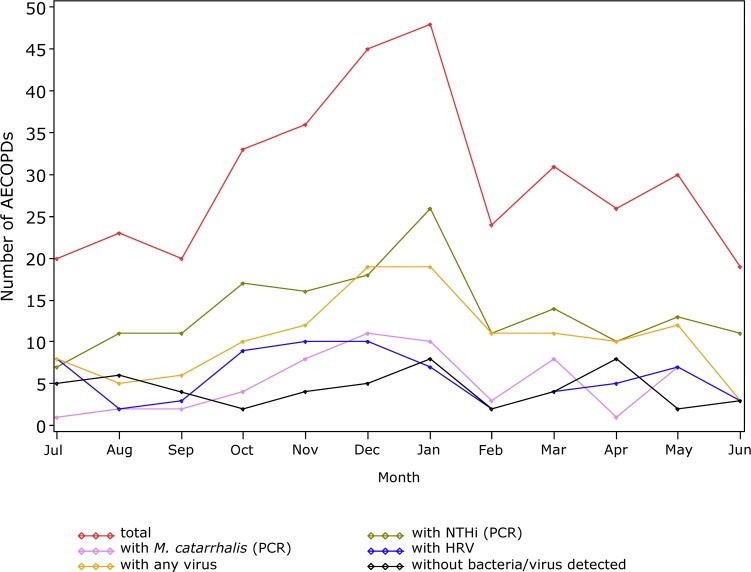
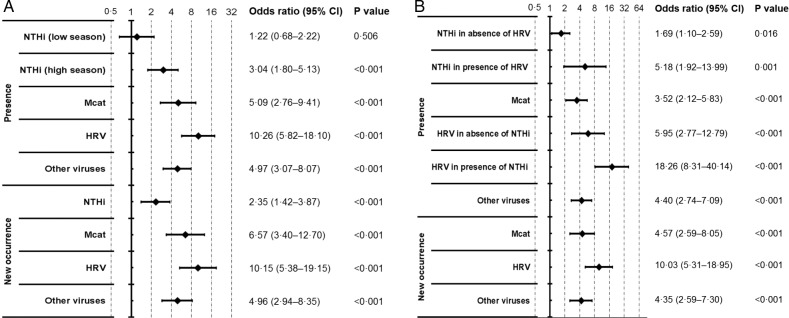
Findings: The mean exacerbation rate per patient-year was 3.04 (95% CI 2.63 to 3.50). At AECOPD, the most common bacterial species were non-typeable Haemophilus influenzae (NTHi) and Moraxella catarrhalis, and the most common virus was rhinovirus. Logistic regression analyses (culture bacterial detection) showed significant OR for AECOPD occurrence when M. catarrhalis was detected regardless of season (5.09 (95% CI 2.76 to 9.41)). When NTHi was detected, the increased risk of exacerbation was greater in high season (October-March, OR 3.04 (1.80 to 5.13)) than low season (OR 1.22 (0.68 to 2.22)). Bacterial and viral coinfection was more frequent at exacerbation (24.9%) than stable state (8.6%). A significant interaction was detected between NTHi and rhinovirus presence and AECOPD risk (OR 5.18 (1.92 to 13.99); p=0.031).
Conclusions: AECOPD aetiology varies with season. Rises in incidence in winter may be driven by increased pathogen presence as well as an interaction between NTHi airway infection and effects of viral infection.
Trial registration number: Results, NCT01360398.
Keywords: Bacterial Infection; COPD Exacerbations; Respiratory Infection; Viral infection.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Competing interests: TMAW has received reimbursement for travel and meeting attendance from Boehringer Ingelheim and AstraZeneca, outside of the submitted work. SB received grants and assistance in travel to conferences from GSK outside of the submitted work. SCC received a grant from Pfizer outside of the submitted work. KJS received grants from Asthma UK (08/026) and BMA HC Roscoe Award outside of the submitted work, and he has a patent PCT/GB2010/050821 ‘Ex Vivo Modelling of Therapeutic Interventions’ pending. EA, J-MD, SS and TGP are employees of the GSK group of companies. MP was an employee of the GSK group of companies at the time the study was conducted. EA, J-MD, SS and TGP hold shares/restricted shares in the GSK group of companies. KJS, VK, NW, KO, SW and TMAW received an institutional grant from the GSK group of companies to conduct this study. AW and AT declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical