

ARTEMIDA Trial (A Randomized Trial of Efficacy, 12 Months International Double-Blind Actovegin): A Randomized Controlled Trial to Assess the Efficacy of Actovegin in Poststroke Cognitive Impairment
- PMID: 28432265
- PMCID: PMC5404405
- DOI: 10.1161/STROKEAHA.116.014321
ARTEMIDA Trial (A Randomized Trial of Efficacy, 12 Months International Double-Blind Actovegin): A Randomized Controlled Trial to Assess the Efficacy of Actovegin in Poststroke Cognitive Impairment
Abstract
Background and purpose: Poststroke cognitive impairment is a debilitating consequence of stroke. The aim of this study was to assess whether Actovegin confers cognitive benefit in patients who have had an ischemic stroke.
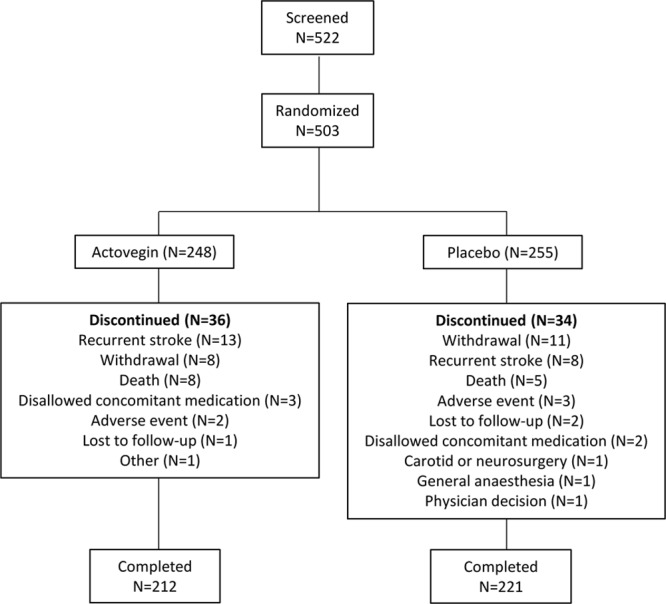
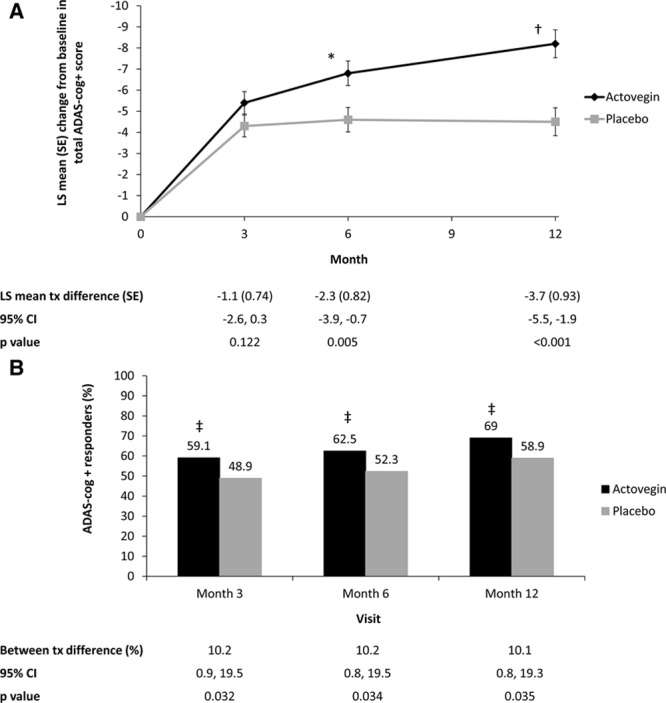
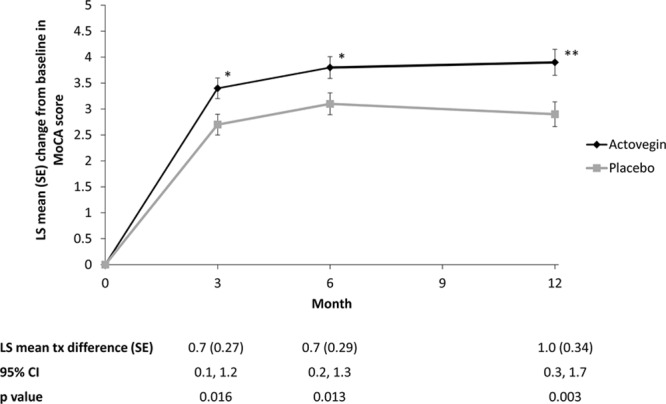
Methods: This was a 12-month, parallel-group, randomized, multicenter, double-blind, placebo-controlled study. Eligible patients were ≥60 years of age with a Montreal Cognitive Assessment test score of ≤25 points. Patients were randomized into 2 groups within 1 week of acute supratentorial ischemic stroke in a 1:1 ratio: Actovegin (a deproteinized hemoderivative of calf blood, 2000 mg/d for ≤20 intravenous infusions followed by 1200 mg/d orally) or placebo for 6 months. Patients were treated in accordance with standard clinical practice for a further 6 months. The primary end point was the change from baseline in Alzheimer's Disease Assessment Scale, cognitive subscale, extended version at 6 months.
Results: Two-hundred forty-eight patients were randomized to Actovegin and 255 patients to placebo. At month 6, the least squares mean change from baseline in Alzheimer's Disease Assessment Scale, cognitive subscale, extended version was -6.8 for Actovegin and -4.6 for placebo; the estimated treatment difference was -2.3 (95% confidence interval, -3.9, -0.7; P=0.005). Recurrent ischemic stroke was the most frequently reported serious adverse event, with a nonsignificantly higher number for Actovegin versus placebo.
Conclusions: Actovegin had a beneficial effect on cognitive outcomes in patients with poststroke cognitive impairment. The safety experience was consistent with the known safety and tolerability profile of the drug. These results warrant confirmation in additional robustly designed studies.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT01582854.
Keywords: Actovegin; post-stroke cognitive impairment; stroke; vascular dementia.
© 2017 The Authors.
Figures
References
-
- Feigin VL, Forouzanfar MH, Krishnamurthi R, Mensah GA, Connor M, Bennett DA, et al. Global Burden of Diseases, Injuries, and Risk Factors Study 2010 (GBD 2010) and the GBD Stroke Experts Group. Global and regional burden of stroke during 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet. 2014;383:245–254. doi: 10.1016/S0140-6736(13)61953-4. - PMC - PubMed
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - PMC - PubMed
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2197–2223. doi: 10.1016/S0140-6736(12)61689-4. - PubMed
-
- Pendlebury ST, Rothwell PM. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: a systematic review and meta-analysis. Lancet Neurol. 2009;8:1006–1018. doi: 10.1016/S1474-4422(09)70236-4. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
