

Evolution and patterns of global health financing 1995-2014: development assistance for health, and government, prepaid private, and out-of-pocket health spending in 184 countries
- PMID: 28433256
- PMCID: PMC5440770
- DOI: 10.1016/S0140-6736(17)30874-7
Evolution and patterns of global health financing 1995-2014: development assistance for health, and government, prepaid private, and out-of-pocket health spending in 184 countries
Abstract
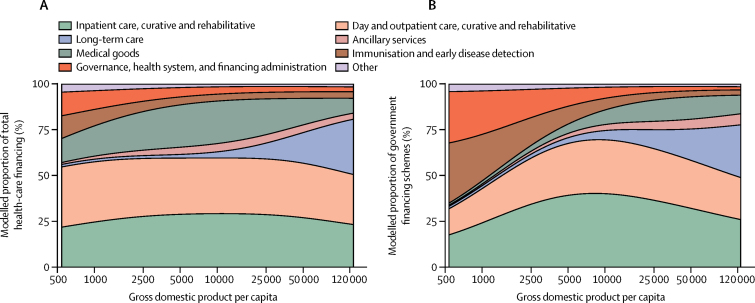
Background: An adequate amount of prepaid resources for health is important to ensure access to health services and for the pursuit of universal health coverage. Previous studies on global health financing have described the relationship between economic development and health financing. In this study, we further explore global health financing trends and examine how the sources of funds used, types of services purchased, and development assistance for health disbursed change with economic development. We also identify countries that deviate from the trends.
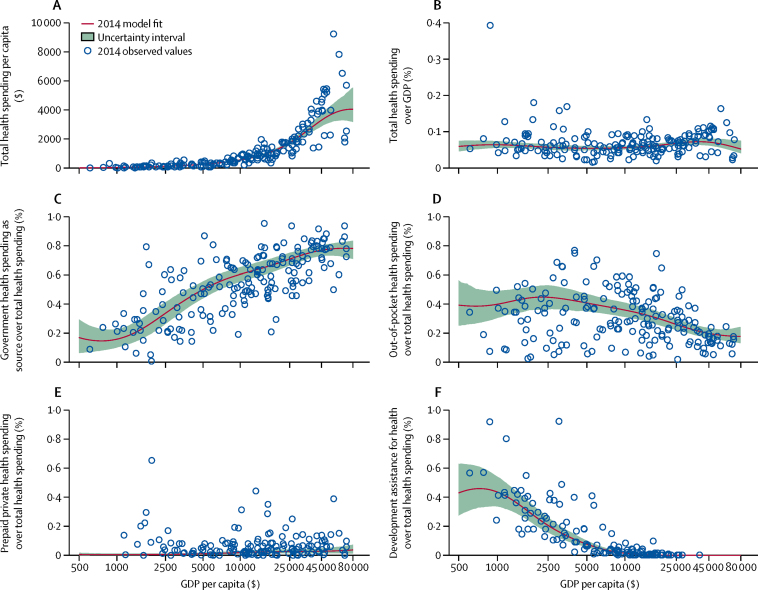
Methods: We estimated national health spending by type of care and by source, including development assistance for health, based on a diverse set of data including programme reports, budget data, national estimates, and 964 National Health Accounts. These data represent health spending for 184 countries from 1995 through 2014. We converted these data into a common inflation-adjusted and purchasing power-adjusted currency, and used non-linear regression methods to model the relationship between health financing, time, and economic development.
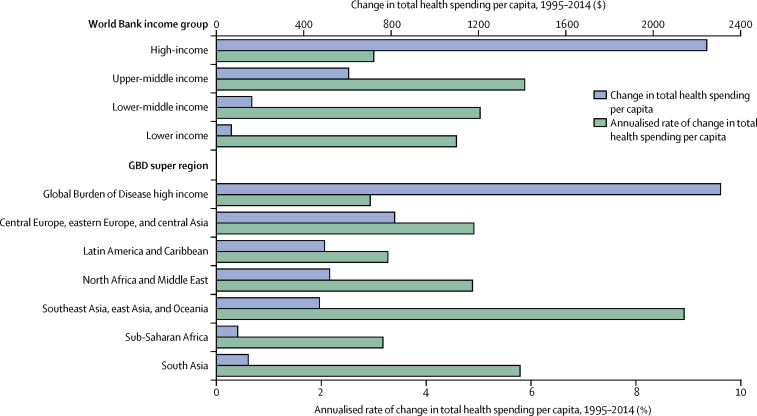
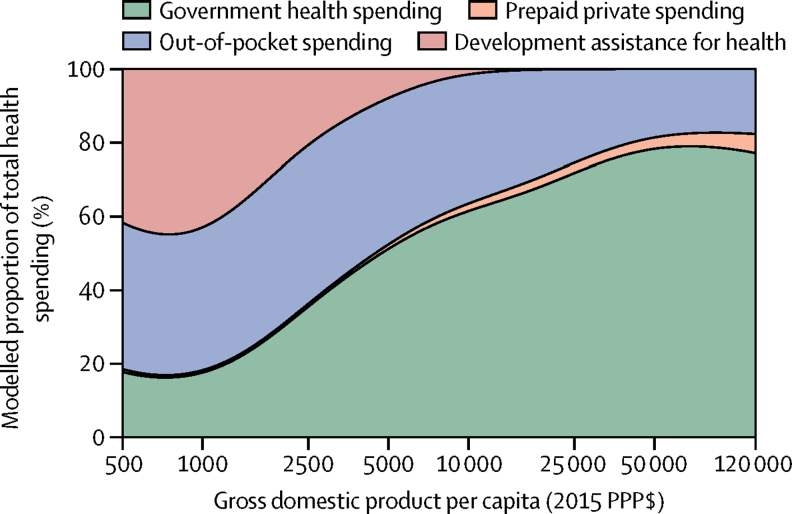
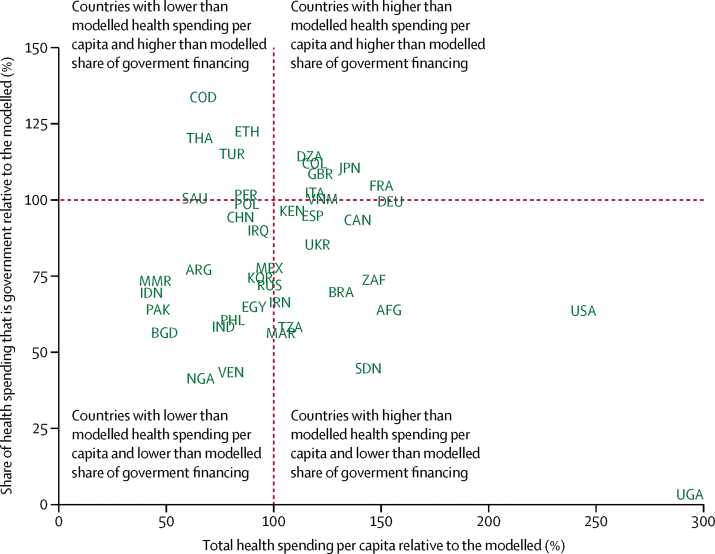
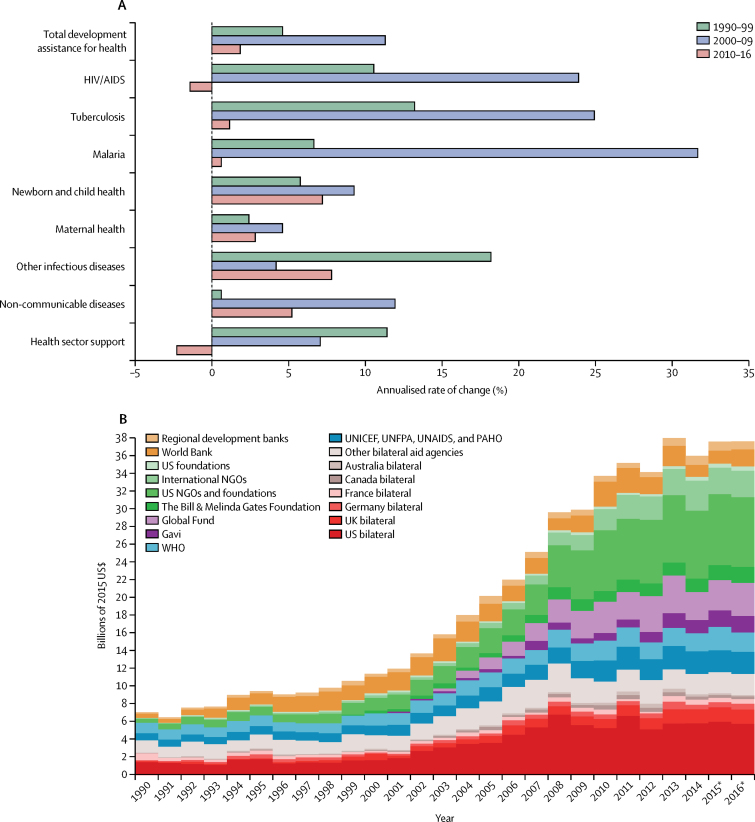
Findings: Between 1995 and 2014, economic development was positively associated with total health spending and a shift away from a reliance on development assistance and out-of-pocket (OOP) towards government spending. The largest absolute increase in spending was in high-income countries, which increased to purchasing power-adjusted $5221 per capita based on an annual growth rate of 3·0%. The largest health spending growth rates were in upper-middle-income (5·9) and lower-middle-income groups (5·0), which both increased spending at more than 5% per year, and spent $914 and $267 per capita in 2014, respectively. Spending in low-income countries grew nearly as fast, at 4·6%, and health spending increased from $51 to $120 per capita. In 2014, 59·2% of all health spending was financed by the government, although in low-income and lower-middle-income countries, 29·1% and 58·0% of spending was OOP spending and 35·7% and 3·0% of spending was development assistance. Recent growth in development assistance for health has been tepid; between 2010 and 2016, it grew annually at 1·8%, and reached US$37·6 billion in 2016. Nonetheless, there is a great deal of variation revolving around these averages. 29 countries spend at least 50% more than expected per capita, based on their level of economic development alone, whereas 11 countries spend less than 50% their expected amount.
Interpretation: Health spending remains disparate, with low-income and lower-middle-income countries increasing spending in absolute terms the least, and relying heavily on OOP spending and development assistance. Moreover, tremendous variation shows that neither time nor economic development guarantee adequate prepaid health resources, which are vital for the pursuit of universal health coverage.
Funding: The Bill & Melinda Gates Foundation.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Patterns of global health financing and potential future spending on health.Lancet. 2017 May 20;389(10083):1955-1956. doi: 10.1016/S0140-6736(17)31001-2. Epub 2017 Apr 20. Lancet. 2017. PMID: 28433257 No abstract available.
References
-
- Gottret P, Schieber G. Health financing revisited. A practitioner's guide. The World Bank; Washington DC: 2006.
-
- Emanuel E, Tanden N, Altman S. A systemic approach to containing health care spending. N Engl J Med. 2012;367:949–954. - PubMed
-
- Center for American Progress Cutting health care costs. Leading experts propose bold solutions. 2012. https://www.americanprogress.org/issues/healthcare/news/2012/08/02/11970... (accessed Dec 5, 2016).
-
- Herman B. Healthcare spending growth rate rises again in 2015. Mod. Healthc. 2016. http://www.modernhealthcare.com/article/20160713/news/160719963 (accessed Dec 5, 2016).
-
- United Nations Population Fund The Prime Minister of Tanzania calls on regional leaders to increase health spending to 15 per cent of national budgets and to strive for achieving health MDGs. 2007. http://www.unfpa.org/press/prime-minister-tanzania-calls-regional-leader... (accessed Dec 6, 2016).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
