

Late renal toxicity of treatment for childhood malignancy: risk factors, long-term outcomes, and surveillance
- PMID: 28434047
- PMCID: PMC5769827
- DOI: 10.1007/s00467-017-3662-z
Late renal toxicity of treatment for childhood malignancy: risk factors, long-term outcomes, and surveillance
Abstract
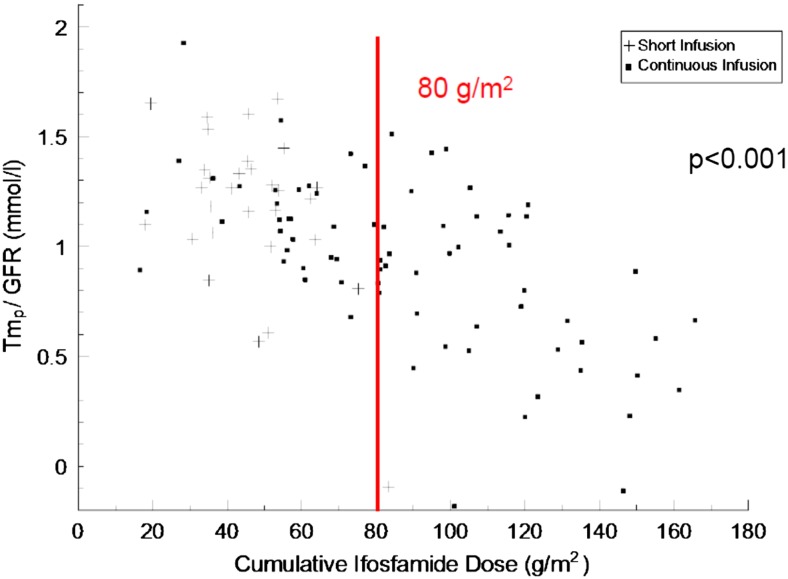
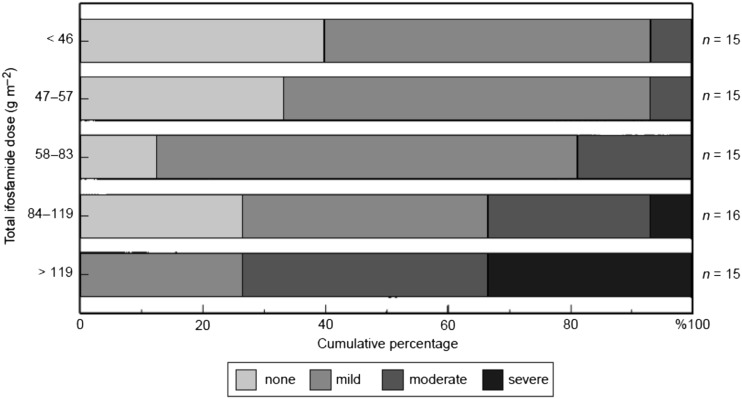
Chronic glomerular and tubular nephrotoxicity is reported in 20-50% and 20-25%, respectively, of children and adolescents treated with ifosfamide and 60-80% and 10-30%, respectively, of those given cisplatin. Up to 20% of children display evidence of chronic glomerular damage after unilateral nephrectomy for a renal tumour. Overall, childhood cancer survivors have a ninefold higher risk of developing renal failure compared with their siblings. Such chronic nephrotoxicity may have multiple causes, including chemotherapy, radiotherapy exposure to kidneys, renal surgery, supportive care drugs and tumour-related factors. These cause a wide range of chronic glomerular and tubular toxicities, often with potentially severe clinical sequelae. Many risk factors for developing nephrotoxicity, mostly patient and treatment related, have been described, but we remain unable to predict all episodes of renal damage. This implies that other factors may be involved, such as genetic polymorphisms influencing drug metabolism. Although our knowledge of the long-term outcomes of chronic nephrotoxicity is increasing, there is still much to learn, including how we can optimally predict or achieve early detection of nephrotoxicity. Greater understanding of the pathogenesis of nephrotoxicity is needed before its occurrence can be prevented.
Keywords: Glomerular toxicity; Ifosfamide; Nephrectomy; Nephrotoxicity; Platinum agents; Renal radiotherapy; Renal tubular toxicity.
Conflict of interest statement
The author declares that he has no conflict of interest.
Figures
References
-
- Oeffinger KC, Mertens AC, Sklar CA, Kawashima T, Hudson MM, Meadows AT, Friedman DL, Marina N, Hobbie W, Kadan-Lottick NS, Schwartz CL, Leisenring W, Robison LL. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006;355:1572–1582. doi: 10.1056/NEJMsa060185. - DOI - PubMed
-
- Skinner R. Nephrotoxicity of cancer treatment in children. Pediatr Health. 2010;4:519–538. doi: 10.2217/phe.10.60. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
