

Aneurysmal Subarachnoid Hemorrhage
- PMID: 28434443
- PMCID: PMC5624452
- DOI: 10.3238/arztebl.2017.0226
Aneurysmal Subarachnoid Hemorrhage
Abstract
Background: Aneurysmal subarachnoid hemorrhage (SAH) is associated with a mortality of more than 30%. Only about 30% of patients with SAB recover sufficiently to return to independent living.
Methods: This article is based on a selective review of pertinent literature retrieved by a PubMed search.
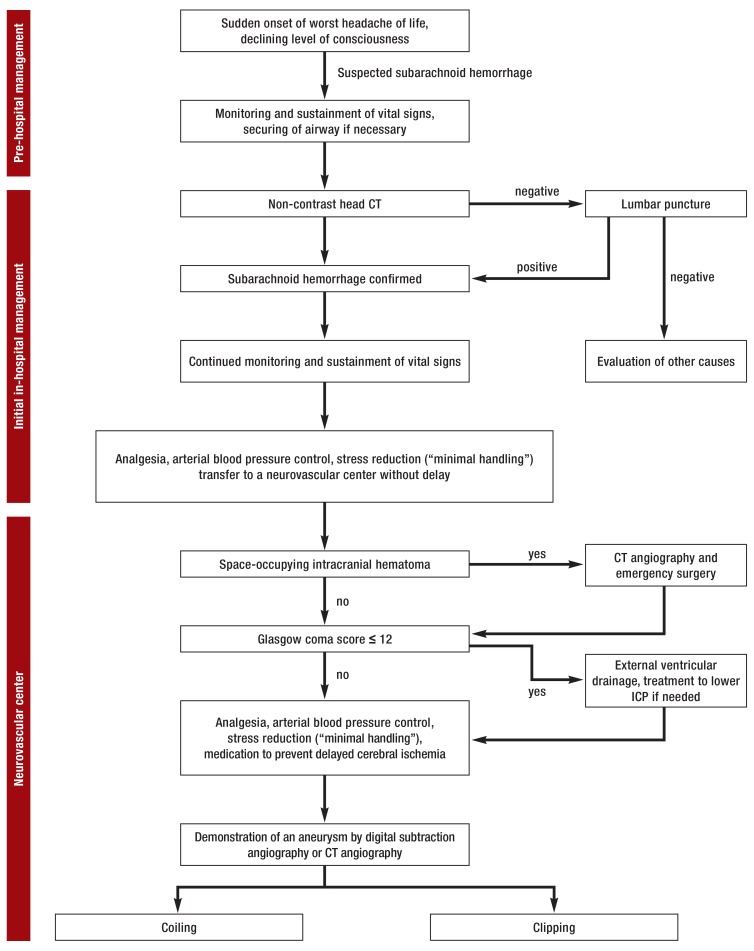
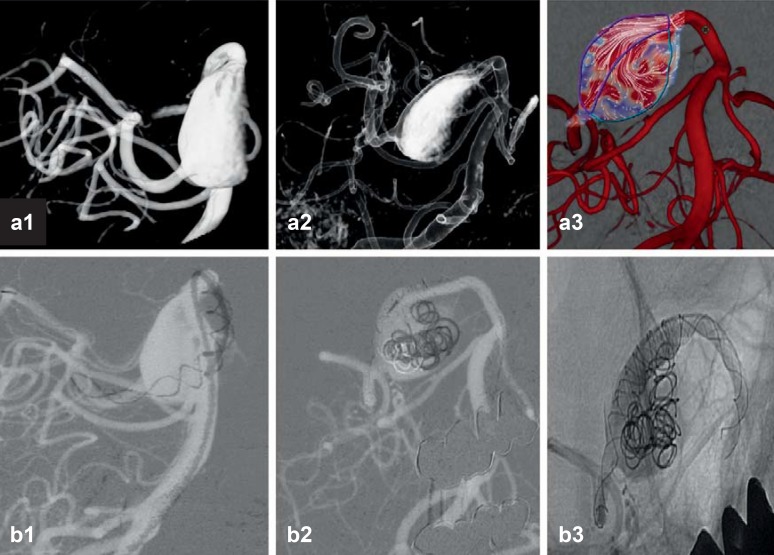
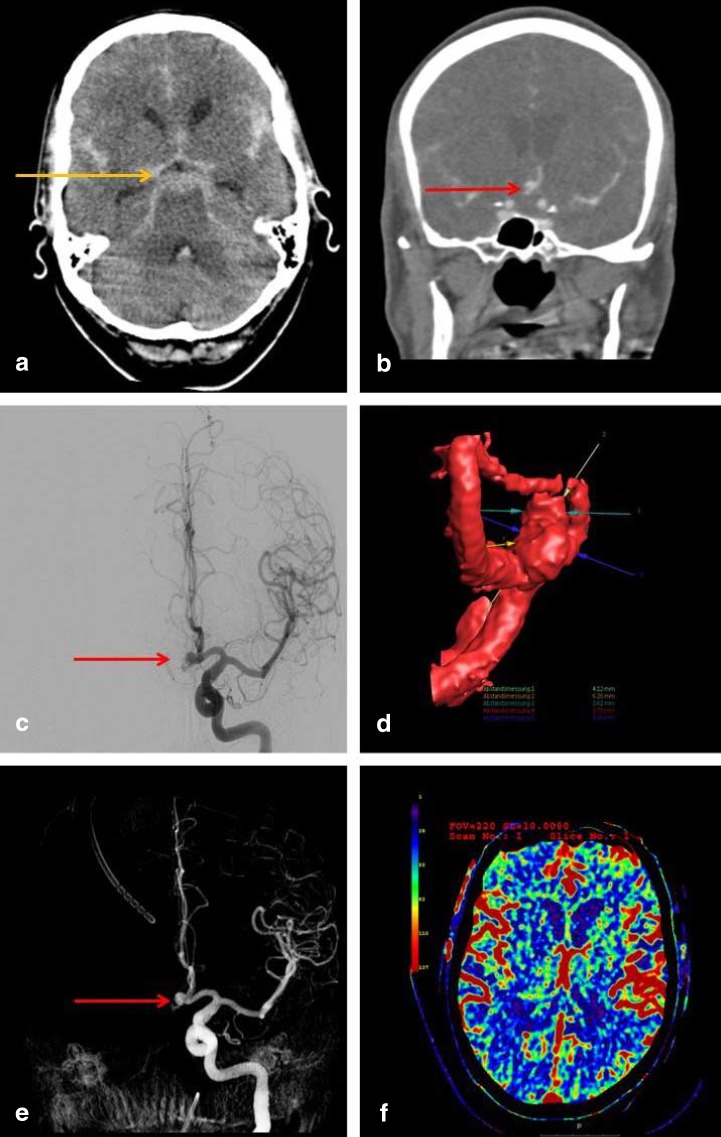
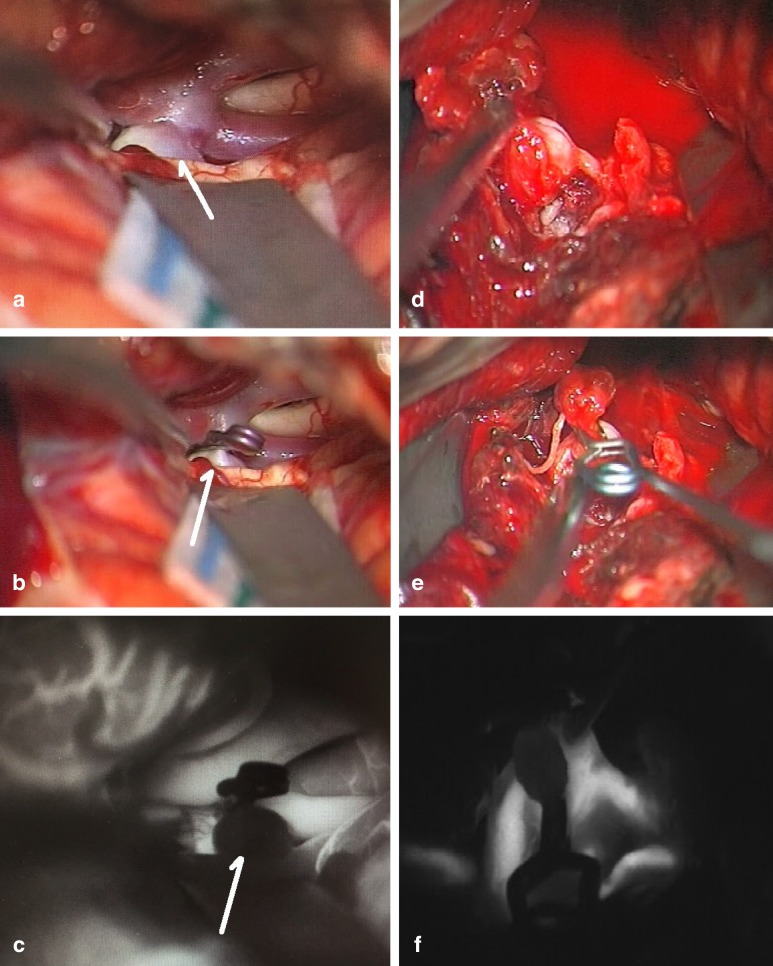
Results: Acute, severe headache, typically described as the worst headache of the patient's life, and meningismus are the characteristic manifestations of SAH. Computed tomog raphy (CT) reveals blood in the basal cisterns in the first 12 hours after SAH with approximately 95% sensitivity and specificity. If no blood is seen on CT, a lumbar puncture must be performed to confirm or rule out the diagnosis of SAH. All patients need intensive care so that rebleeding can be avoided and the sequelae of the initial bleed can be minimized. The immediate transfer of patients with acute SAH to a specialized center is crucially important for their outcome. In such centers, cerebral aneurysms can be excluded from the circulation either with an interventional endovascular procedure (coiling) or by microneurosurgery (clipping).
Conclusion: SAH is a life-threatening condition that requires immediate diagnosis, transfer to a neurovascular center, and treatment without delay.
Figures
References
-
- Molyneux AJ, Kerr RS, Yu LM, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet. 2005;366:809–817. - PubMed
-
- Wiebers DO, Whisnant JP, Huston J, et al. 3rd Unruptured intracranial aneurysms: Natural history, clinical outcome, and risks of surgical and endovascular treatment. International study of unruptured intracranial aneurysms investigators. Lancet. 2003;362:103–110. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical