

Melorheostosis: Exome sequencing of an associated dermatosis implicates postzygotic mosaicism of mutated KRAS
- PMID: 28434888
- PMCID: PMC5518630
- DOI: 10.1016/j.bone.2017.04.010
Melorheostosis: Exome sequencing of an associated dermatosis implicates postzygotic mosaicism of mutated KRAS
Abstract
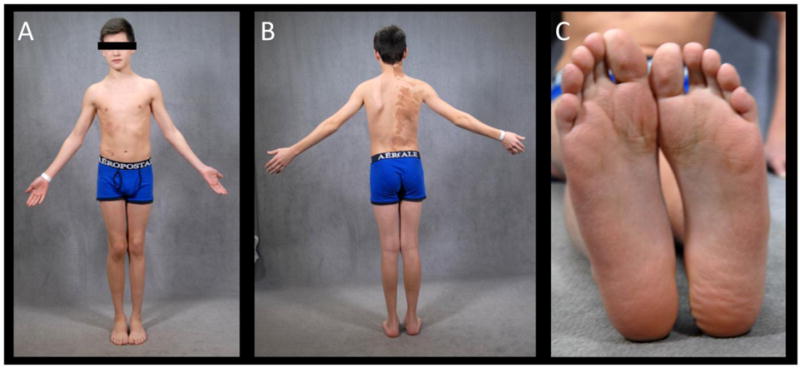
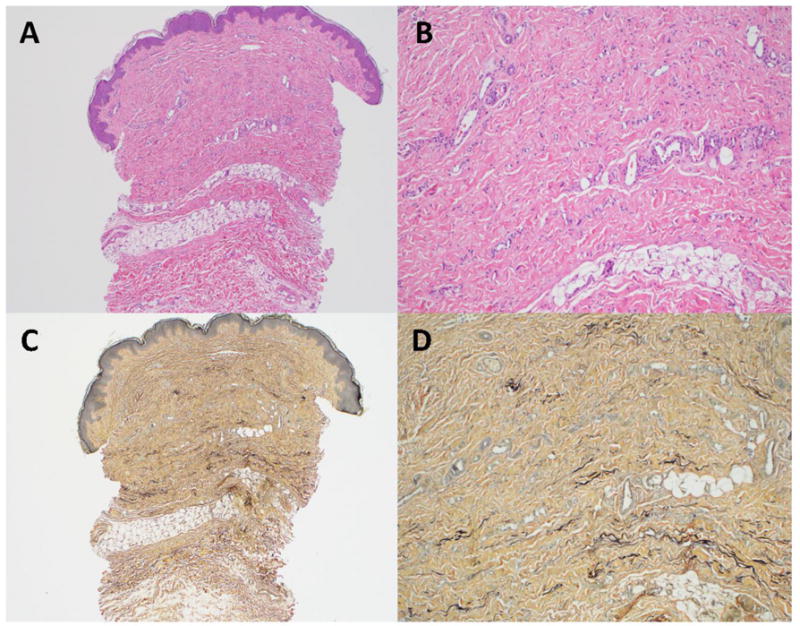
Melorheostosis (MEL) is the rare sporadic dysostosis characterized by monostotic or polyostotic osteosclerosis and hyperostosis often distributed in a sclerotomal pattern. The prevailing hypothesis for MEL invokes postzygotic mosaicism. Sometimes scleroderma-like skin changes, considered a representation of the pathogenetic process of MEL, overlie the bony changes, and sometimes MEL becomes malignant. Osteopoikilosis (OPK) is the autosomal dominant skeletal dysplasia that features symmetrically distributed punctate osteosclerosis due to heterozygous loss-of-function mutation within LEMD3. Rarely, radiographic findings of MEL occur in OPK. However, germline mutation of LEMD3 does not explain sporadic MEL. To explore if mosaicism underlies MEL, we studied a boy with polyostotic MEL and characteristic overlying scleroderma-like skin, a few bony lesions consistent with OPK, and a large epidermal nevus known to usually harbor a HRAS, FGFR3, or PIK3CA gene mutation. Exome sequencing was performed to ~100× average read depth for his two dermatoses, two areas of normal skin, and peripheral blood leukocytes. As expected for non-malignant tissues, the patient's mutation burden in his normal skin and leukocytes was low. He, his mother, and his maternal grandfather carried a heterozygous, germline, in-frame, 24-base-pair deletion in LEMD3. Radiographs of the patient and his mother revealed bony foci consistent with OPK, but she showed no MEL. For the patient, somatic variant analysis, using four algorithms to compare all 20 possible pairwise combinations of his five DNA samples, identified only one high-confidence mutation, heterozygous KRAS Q61H (NM_033360.3:c.183A>C, NP_203524.1:p.Gln61His), in both his dermatoses but absent in his normal skin and blood. Thus, sparing our patient biopsy of his MEL bone, we identified a heterozygous somatic KRAS mutation in his scleroderma-like dermatosis considered a surrogate for MEL. This implicates postzygotic mosaicism of mutated KRAS, perhaps facilitated by germline LEMD3 haploinsufficiency, causing his MEL.
Keywords: Dysostosis; Hyperostosis; LEMD3; Linear epidermal nevus; Malignancy; Nevus sebaceous; Osteopoikilosis; Osteosclerosis; Scleroderma; TGFβ.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures





Similar articles
-
Deactivating germline mutations in LEMD3 cause osteopoikilosis and Buschke-Ollendorff syndrome, but not sporadic melorheostosis.J Bone Miner Res. 2007 Feb;22(2):243-50. doi: 10.1359/jbmr.061102. J Bone Miner Res. 2007. PMID: 17087626
-
Melorheostosis and Osteopoikilosis Clinical and Molecular Description of an Italian Case Series.Calcif Tissue Int. 2019 Aug;105(2):215-221. doi: 10.1007/s00223-019-00565-6. Epub 2019 May 25. Calcif Tissue Int. 2019. PMID: 31129707
-
Germline LEMD3 mutations are rare in sporadic patients with isolated melorheostosis.Hum Mutat. 2006 Mar;27(3):290. doi: 10.1002/humu.9403. Hum Mutat. 2006. PMID: 16470551
-
Melorheostosis and Osteopoikilosis: A Review of Clinical Features and Pathogenesis.Calcif Tissue Int. 2019 May;104(5):530-543. doi: 10.1007/s00223-019-00543-y. Epub 2019 Apr 15. Calcif Tissue Int. 2019. PMID: 30989250 Review.
-
Schimmelpenning-Feuerstein-Mims syndrome induced by HRAS Gly12Ser somatic mosaic mutation: Case report and literature review.J Dermatol. 2023 Sep;50(9):1213-1215. doi: 10.1111/1346-8138.16822. Epub 2023 May 12. J Dermatol. 2023. PMID: 37170693 Review.
Cited by
-
Lymphatic Malformation Responsive to Sirolimus in Keratinocytic Epidermal Nevus Syndrome with KRAS Mutation: A Case and Brief Literature Discussion.Case Rep Dermatol. 2021 Apr 1;13(1):195-201. doi: 10.1159/000515247. eCollection 2021 Jan-Apr. Case Rep Dermatol. 2021. PMID: 34703427 Free PMC article.
-
Case Report: Sequential postzygotic HRAS mutation and gains of the paternal chromosome 11 carrying the mutated allele in a patient with epidermal nevus and rhabdomyosarcoma: evidence of a multiple-hit mechanism involving HRAS in oncogenic transformation.Front Genet. 2023 Aug 10;14:1231434. doi: 10.3389/fgene.2023.1231434. eCollection 2023. Front Genet. 2023. PMID: 37636262 Free PMC article.
-
Distinct Clinical and Pathological Features of Melorheostosis Associated With Somatic MAP2K1 Mutations.J Bone Miner Res. 2019 Jan;34(1):145-156. doi: 10.1002/jbmr.3577. Epub 2018 Sep 14. J Bone Miner Res. 2019. PMID: 30138550 Free PMC article. Clinical Trial.
-
Late-Onset Melorheostosis: A Case Report.Case Rep Oncol. 2023 Oct 26;16(1):1237-1244. doi: 10.1159/000534241. eCollection 2023 Jan-Dec. Case Rep Oncol. 2023. PMID: 38130895 Free PMC article.
-
Clinical Evaluation of Melorheostosis in the Context of a Natural History Clinical Study.JBMR Plus. 2019 Jul 26;3(8):e10214. doi: 10.1002/jbm4.10214. eCollection 2019 Aug. JBMR Plus. 2019. PMID: 31485554 Free PMC article.
References
-
- Online Mendelian Inheritance in Man, OMIM®. McKusick-Nathans Institute of Genetic Medicine, Johns Hopkins University; Baltimore, MD: Dec, 2016. World Wide Web URL http://omim.org.
-
- Perlman MD. Melorheostosis: A case report and literature review. J Foot Surg. 1990;29:353–6. - PubMed
-
- Greenspan A, Azouz EM. Bone dysplasia series. Melorheostosis: Review and update. Can Assoc Radiol J. 1999;50:324–30. - PubMed
-
- Freyschmidt J. Melorheostosis: A review of 23 cases. Eur Radiol. 2001;11:474–9. - PubMed
-
- Thompson NM, Andrews GC, Gillwald FN. Scleroderma and melorheostosis: report of a case. J Bone Jt Surg. 1951;33-B:430–3. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
