

Evaluation of EX-PRESS glaucoma implant in elderly diabetic patients after 23G vitrectomy
- PMID: 28435237
- PMCID: PMC5391864
- DOI: 10.2147/CIA.S128618
Evaluation of EX-PRESS glaucoma implant in elderly diabetic patients after 23G vitrectomy
Abstract
Purpose: The most frequent qualifications for pars plana vitrectomy (PPV) in diabetic patients include recurrent hemorrhage into the vitreous body chamber and vitreoretinal proliferation, also with traction retinal detachment. The aim of this study was to evaluate the effectiveness of EX-PRESS implant for the treatment of secondary glaucoma in elderly diabetic patients following PPV 23G with silicon oil or SF6 gas endotamponade.
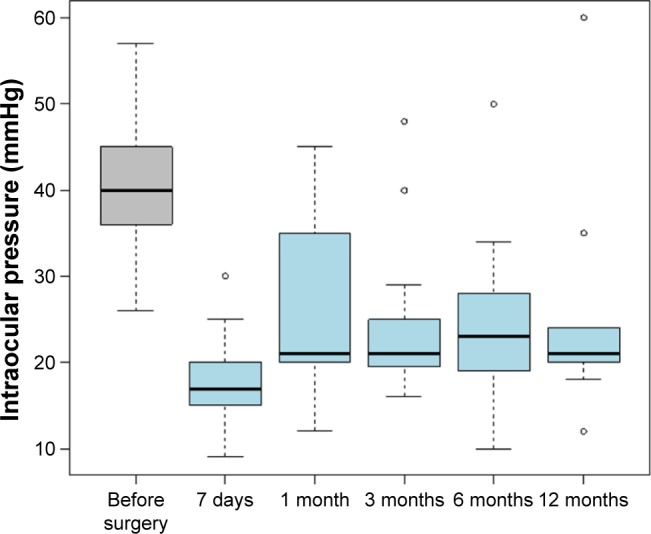
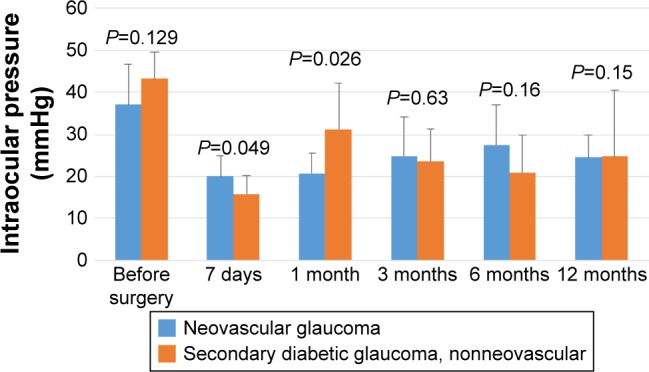
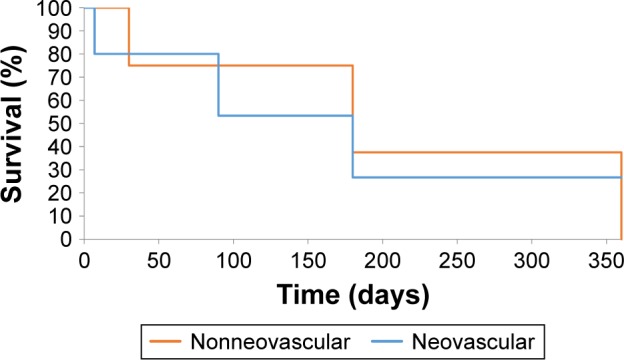
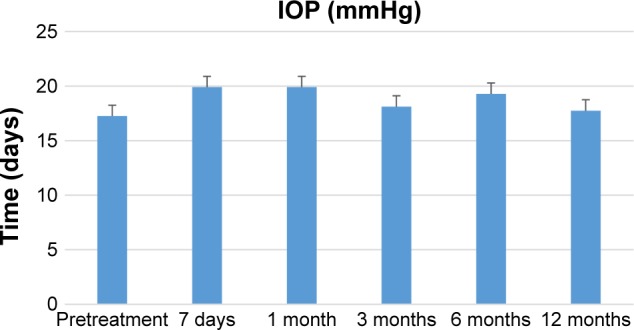
Materials and methods: This retrospective analysis comprised 18 patients (19 eyes). We applied EX-PRESS implants in 9 patients with neovascular glaucoma (NVG) and in 10 patients with non-NVG. All patients had earlier history of diabetes and vitrectomy 23G for diabetic complications. Intraocular pressure (IOP) was measured and compared before; 7 days; 1, 3, 6, and 12 months; and a year after the surgery.
Results: Application of the implant exhibited a lowering effect on IOP. After 1 month, 53% of patients had IOP values beyond 22 mmHg, while 86% after 1 year.
Conclusion: The implant can be used to treat both NVG and non-NVG in diabetic patients following PPV.
Keywords: DM; IOP; PPV; glaucoma surgery.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27(5):1047–1053. - PubMed
-
- Fong DS, Aiello L, Gardner TW, et al. Retinopathy in diabetes. Diabetes Care. 2004;27(suppl 1):S84–S87. - PubMed
-
- Samuelson TW, Stamper R, Gallardo M. Flow dynamics of the EX-PRESS® glaucoma filtration device. US Ophthalmic Rev. 2014;7(1):39.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
