

Security, Violent Events, and Anticipated Surge Capabilities of Emergency Departments in Washington State
- PMID: 28435498
- PMCID: PMC5391897
- DOI: 10.5811/westjem.2016.10.30271
Security, Violent Events, and Anticipated Surge Capabilities of Emergency Departments in Washington State
Abstract
Introduction: Over the past 15 years, violent threats and acts against hospital patients, staff, and providers have increased and escalated. The leading area for violence is the emergency department (ED) given its 24/7 operations, role in patient care, admissions gateway, and center for influxes during acute surge events. This investigation had three objectives: to assess the current security of Washington State EDs; to estimate the prevalence of and response to threats and violence in Washington State EDs; and to appraise the Washington State ED security capability to respond to acute influxes of patients, bystanders, and media during acute surge events.
Methods: A voluntary, blinded, 28-question Web-based survey developed by emergency physicians was electronically delivered to all 87 Washington State ED directors in January 2013. We evaluated responses by descriptive statistical analyses.
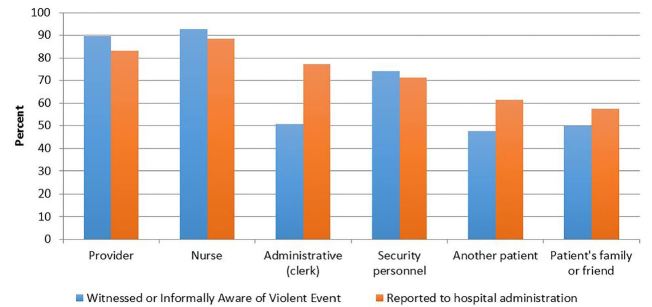
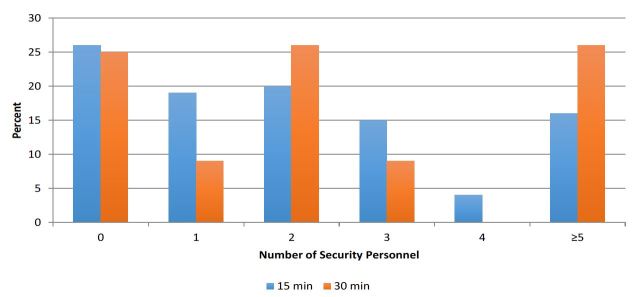
Results: Analyses occurred after 90% (78/87) of ED directors responded. Annual censuses of the EDs ranged from < 20,000 to 100,000 patients and represented the entire spectrum of practice environments, including critical access hospitals and a regional quaternary referral medical center. Thirty-four of 75 (45%) reported the current level of security was inadequate, based on the general consensus of their ED staff. Nearly two-thirds (63%) of EDs had 24-hour security personnel coverage, while 28% reported no assigned security personnel. Security personnel training was provided by 45% of hospitals or healthcare systems. Sixty-nine of 78 (88%) respondents witnessed or heard about violent threats or acts occurring in their ED. Of these, 93% were directed towards nursing staff, 90% towards physicians, 74% towards security personnel, and 51% towards administrative personnel. Nearly half (48%) noted incidents directed towards another patient, and 50% towards a patient's family or friend. These events were variably reported to the hospital administration. After an acute surge event, 35% believed the initial additional security response would not be adequate, with 26% reporting no additional security would be available within 15 minutes.
Conclusion: Our study reveals the variability of ED security staffing and a heterogeneity of capabilities throughout Washington State. These deficiencies and vulnerabilities highlight the need for other EDs and regional emergency preparedness planners to conduct their own readiness assessments.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The views expressed are those of the authors and do not reflect the official policy of the Department of the Army, the Department of Defense, or the US Government.
Figures
Similar articles
-
Violent events and security programs in California Emergency Departments before and after the 1993 Hospital Security Act.J Emerg Nurs. 2002 Oct;28(5):420-6. doi: 10.1067/men.2002.127567. J Emerg Nurs. 2002. PMID: 12386623
-
Waterworks, a full-scale chemical exposure exercise: interrogating pediatric critical care surge capacity in an inner-city tertiary care medical center.Prehosp Disaster Med. 2014 Feb;29(1):100-6. doi: 10.1017/S1049023X13009096. Epub 2013 Dec 13. Prehosp Disaster Med. 2014. PMID: 24330801
-
Pandemic influenza and major disease outbreak preparedness in US emergency departments: a survey of medical directors and department chairs.Am J Disaster Med. 2009 Jul-Aug;4(4):199-206. Am J Disaster Med. 2009. PMID: 19860162
-
Security interventions for workplace violence in the emergency department.Emerg Med Australas. 2018 Dec;30(6):802-807. doi: 10.1111/1742-6723.13093. Epub 2018 Jun 25. Emerg Med Australas. 2018. PMID: 30129701 Review.
-
Security in pediatric emergency departments.Pediatr Emerg Care. 1995 Aug;11(4):220-2. doi: 10.1097/00006565-199508000-00007. Pediatr Emerg Care. 1995. PMID: 8532566 Review.
Cited by
-
Characteristics of Workplace Violence on Doctors and Nurses at the Accident and Emergency Department in a Southern State of Nigeria.Niger Med J. 2023 Jul 2;64(3):398-407. eCollection 2023 May-Jun. Niger Med J. 2023. PMID: 38974071 Free PMC article.
-
Unheard Victims: Multidisciplinary Incidence and Reporting of Violence in an Emergency Department.West J Emerg Med. 2021 May 7;22(3):702-709. doi: 10.5811/westjem.2021.2.50046. West J Emerg Med. 2021. PMID: 34125050 Free PMC article.
-
Workplace Violence in the Emergency Department: Case Study on Staff and Law Enforcement Disagreement on Reportable Crimes.Int J Environ Res Public Health. 2022 Jun 2;19(11):6818. doi: 10.3390/ijerph19116818. Int J Environ Res Public Health. 2022. PMID: 35682399 Free PMC article.
-
Preferences of healthcare workers for security personnel to prevent occupational violence: A discrete choice experiment.Work. 2025 Aug;81(4):3285-3293. doi: 10.1177/10519815251330539. Epub 2025 Apr 17. Work. 2025. PMID: 40241652 Free PMC article.
References
-
- Sentinel Event Alert 45: Preventing Violence in the health care setting. The Joint Commission; 2010. [Accessed Jan 22, 2015]. Available at: http://www.jointcommission.org/sentinel_event_alert_issue_45_preventing_... - PubMed
-
- National Institute for Occupational Safety and Health. Center for Disease Control and Prevention, NOISH Publications; [Accessed Jan 23, 2015]. Violence: occupational Hazards in Hospitals. Available at: http://www.cdc.gov/niosh/docs/2002-101/
-
- Kelen GD, Catlett CL, Kubit JG, et al. Hospital-based shootings in the United States: 2000 to 2011. Ann Emerg Med. 2012;60(6):790–8.e1. - PubMed
-
- Morganti KG, Bauhott S, Blanchard JC, et al. Research Report: The evolving roles of emergency departments in the United States. The Rand Corporation; 2013. [Accessed Jan 25, 2015]. Available at: http://www.rand.org/pubs/research_reports/RR280.html.
-
- Blando J, McGreevy K, O’Hagan E, et al. Emergency Department Security Programs, Community Crime, and Employee Assaults. J Emerg Med. 2012;42(3):329–38. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous