

Humeral Supracondylar Fractures in Children: A Novel Technique of Lateral External Fixation and Kirschner Wiring
- PMID: 28435560
- PMCID: PMC5333657
- DOI: 10.5704/MOJ.1607.008
Humeral Supracondylar Fractures in Children: A Novel Technique of Lateral External Fixation and Kirschner Wiring
Abstract
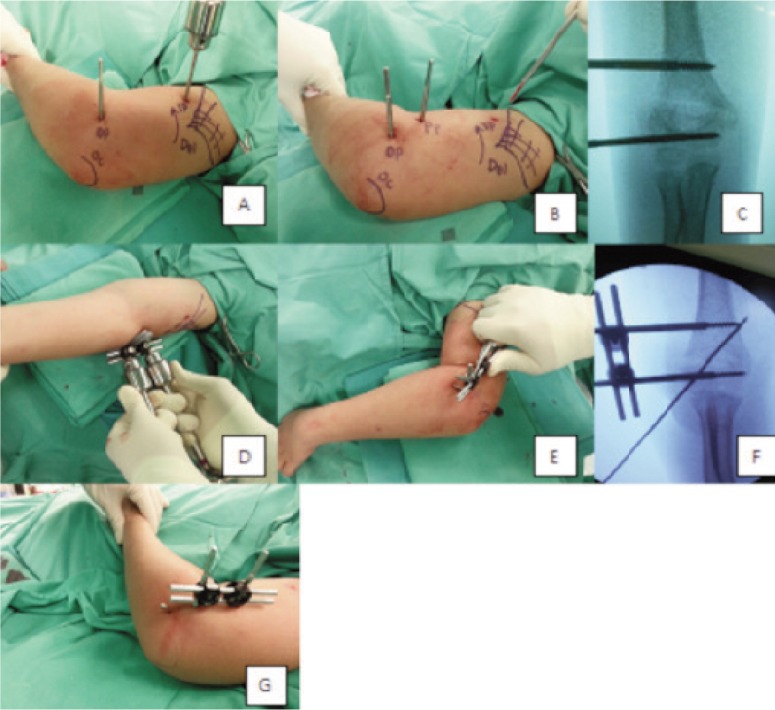
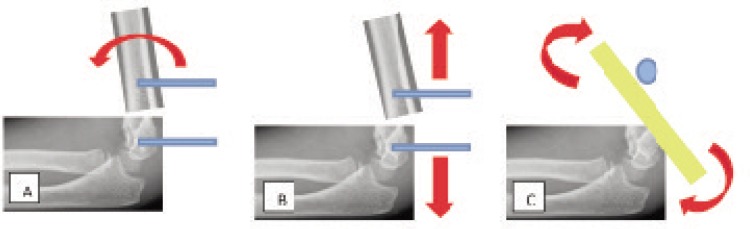
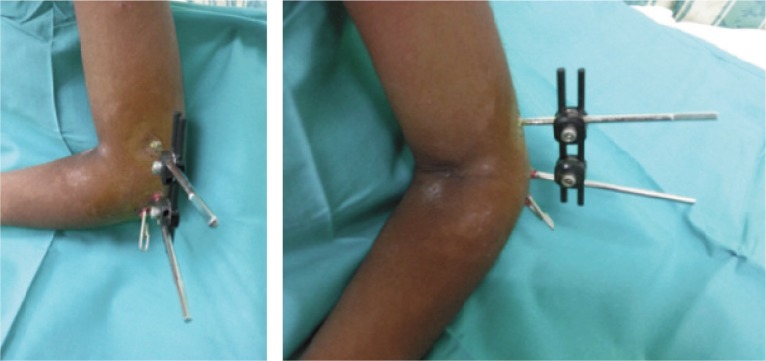
Introduction: Supracondylar fracture of the humerus is the most common fracture around the elbow in children. Pinning with Kirschner wires (K-wires) after open or closed reduction is generally accepted as the primary treatment modality. However, it comes with the risk of persistent instability and if the K-wire is not inserted properly, it may cause displacement and varus deformity. We present our two-year experience with a new technique of lateral external fixation and K-wiring of the humeral supracondylar fracture. Materials and Methods: A total of seven children with irreducible Gartland Type III supracondylar humeral fracture were treated with closed reduction and lateral external fixation and lateral Kirschner wiring. Patients with ipsilateral radial or ulnar fracture, open fracture and presence of neurovascular impairment pre-operatively were excluded. All the patients were followed up at one, three and six weeks and three and six months. The final outcomes were assessed based on Flynn's criteria. Results: All the patients achieved satisfactory outcomes in terms of cosmetic and functional aspects. All patients except one (85.5%) regained excellent and good cosmetic and functional status. One patient (14.3%) sustained pin site infection which resolved with oral antibiotic (Checketts- Otterburn grade 2). There was no neurological deficit involving the ulnar nerve and radial nerve. Conclusion: The introduction of lateral external fixation and lateral percutaneous pinning provide a promising alternative method for the treatment of humeral supracondylar fracture. This study demonstrates that it has satisfactory cosmetic and functional outcomes with no increased risk of complications compared to percutaneous pinning.
Keywords: Kirschner wire; Supracondylar fracture; external fixator; humerus.
Figures


Similar articles
-
Outcome Analysis of Lateral Pinning for Displaced Supracondylar Fractures in Children Using Three Kirschner Wires in Parallel and Divergent Configuration.Indian J Orthop. 2018 Sep-Oct;52(5):554-560. doi: 10.4103/ortho.IJOrtho_462_17. Indian J Orthop. 2018. PMID: 30237614 Free PMC article.
-
Lateral entry pins and Slongo's external fixation: which method is more ideal for older children with supracondylar humeral fractures?J Orthop Surg Res. 2021 Jun 21;16(1):396. doi: 10.1186/s13018-021-02541-z. J Orthop Surg Res. 2021. PMID: 34154623 Free PMC article.
-
Clinical Results of Closed Reduction and Percutaneous Pinning for Gartland Type II Flexion-Type Supracondylar Humeral Fractures in Children: Report of Three Cases.J Nippon Med Sch. 2023;90(3):294-300. doi: 10.1272/jnms.JNMS.2023_90-402. J Nippon Med Sch. 2023. PMID: 37380478
-
Modern Treatment of Supracondylar Humeral Fractures in Children.Children (Basel). 2025 Apr 25;12(5):556. doi: 10.3390/children12050556. Children (Basel). 2025. PMID: 40426735 Free PMC article. Review.
-
Management of pediatric distal humerus metaphyseal-diaphyseal junction fracture: A systematic review and meta-analysis.J Child Orthop. 2024 Jun 22;18(4):421-431. doi: 10.1177/18632521241262169. eCollection 2024 Aug. J Child Orthop. 2024. PMID: 39100985 Free PMC article. Review.
Cited by
-
Can a linear external fixator stand as a surgical alternative to open reduction in treating a high-grade supracondylar humerus fracture?J Int Med Res. 2019 Jan;47(1):133-141. doi: 10.1177/0300060518797022. Epub 2018 Sep 10. J Int Med Res. 2019. PMID: 30198367 Free PMC article.
-
A Comparison of Nerve Injury in Cross Versus Lateral Pinning Fixation of Displaced Supracondylar Humerus Fracture.Cureus. 2024 Sep 28;16(9):e70404. doi: 10.7759/cureus.70404. eCollection 2024 Sep. Cureus. 2024. PMID: 39473689 Free PMC article.
-
Supracondylar Humerus Fractures: Classification Based Treatment Algorithms.Indian J Orthop. 2020 Oct 22;55(1):68-80. doi: 10.1007/s43465-020-00285-2. eCollection 2021 Feb. Indian J Orthop. 2020. PMID: 33569100 Free PMC article. Review.
-
Mechanical stability study of three techniques used in the fixation of transverse and oblique metaphyseal-diaphyseal junction fractures of the distal humerus in children: a finite element analysis.J Orthop Surg Res. 2020 Jan 31;15(1):34. doi: 10.1186/s13018-020-1564-4. J Orthop Surg Res. 2020. PMID: 32020882 Free PMC article.
-
[Research progress in the treatment of distal humeral metaphyseal-diaphyseal junction fracture in children].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 May 15;38(5):613-617. doi: 10.7507/1002-1892.202402044. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 38752250 Free PMC article. Review. Chinese.
References
-
- Chai KK, Saw A, Sengupta S. Supracondylar Fractures of the Humerus in Children – An Epidemiological Study of 132 Consecutive Cases. Med J Malaysia. 2000;55:39–42. - PubMed
-
- Wilkins K, Beaty JH, Chambers HG, Toniolo RM. Fractures and dislocations of the elbow region. In: Rockwood CA, Wilkins KE, Beaty JH, editors. Fractures in children. 4th ed. Philadelphia: Lippincott; 1996. pp. 653–904.
-
- Aktekin CN, Toprak A, Ozturk AM, Altay M, Ozkurt B, Tabak AY. Open reduction via posterior triceps sparing approach in comparison with closed treatment of posteromedial displaced Gartland type III supracondylar humerus fractures. J Pediatr Orthop Br. 2008;17(4):171–8. - PubMed
-
- Gartland JJ. Management of supracondylar fracture of the humerus in children. J Am Acad Orthop Surg. 1997;5:19–26. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources