

Angiofibrolipoma of Posterior Mediastinum with Transforaminal Extension
- PMID: 28435645
- PMCID: PMC5379235
- DOI: 10.4081/rt.2017.6811
Angiofibrolipoma of Posterior Mediastinum with Transforaminal Extension
Abstract
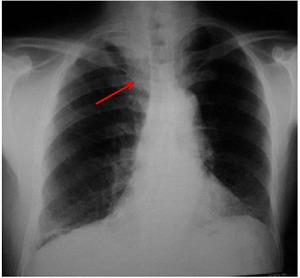
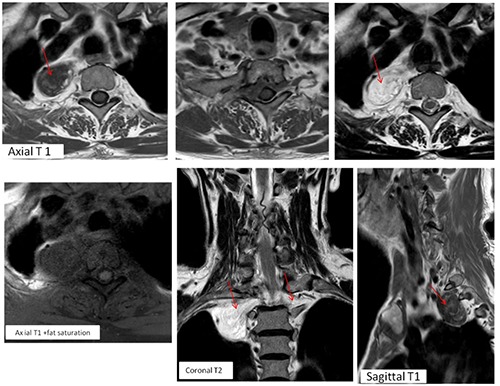
Angiofibrolipoma is a histological variant of lipoma, which commonly occurs in subcutaneous tissues. In the present report we illustrate the case of an angiofibrolipoma of the posterior upper mediastinum in a 75-year-old man presented with progressive chest pain. Xray chest showed a homogeneous opacity vertically oriented along the right lateral aspect of thoracic vertebrae with an obtuse angle to the mediastinum. The upper extremity of the mass extended above the superior clavicle, suggestive of a posterior mediastinal lesion. Thoracic magnetic resonance imaging revealed a posterior mediastinal mass, in keeping with a nonaggressive lesion, with particular endocanalar extension and heterogeneous signal and enhancement patterns that was highly suggestive of a mixed mesenchymal tumor. The tumor was incompletely removed by right postero-lateral thoracotomy with final diagnosis of angiofibrolipoma. To the author's knowledge, such a case of angiofibrolipoma located in the posterior mediastinum has not been previously reported in the literature.
Keywords: Angiofibrolipoma; MRI; Mesenchymal tumors; Posterior mediastinum.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
