

Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients
- PMID: 28435689
- PMCID: PMC5395899
- DOI: 10.1186/s40814-015-0006-2
Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients
Abstract
Background: Selecting positive end-expiratory pressure (PEEP) during mechanical ventilation is important, as it can influence disease progression and outcome of acute respiratory distress syndrome (ARDS) patients. However, there are no well-established methods for optimizing PEEP selection due to the heterogeneity of ARDS. This research investigates the viability of titrating PEEP to minimum elastance for mechanically ventilated ARDS patients.
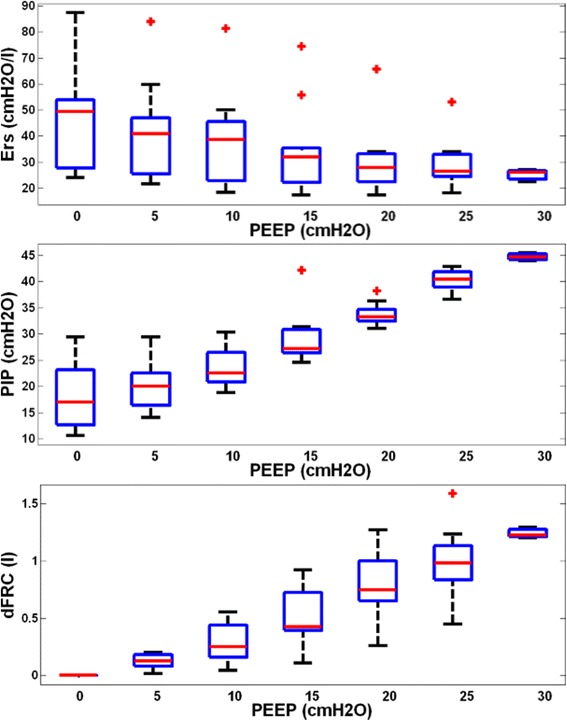
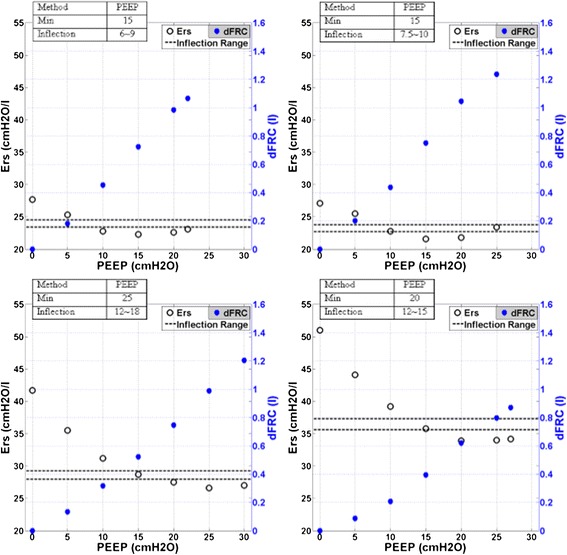
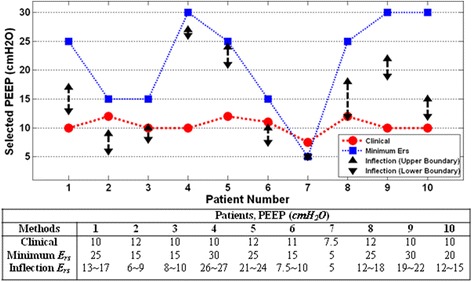
Methods: Ten mechanically ventilated ARDS patients from the Christchurch Hospital Intensive Care Unit were included in this study. Each patient underwent a stepwise PEEP recruitment manoeuvre. Airway pressure and flow data were recorded using a pneumotachometer. Patient-specific respiratory elastance (Ers ) and dynamic functional residual capacity (dFRC) at each PEEP level were calculated and compared. Optimal PEEP for each patient was identified by finding the minima of the PEEP-Ers profile.
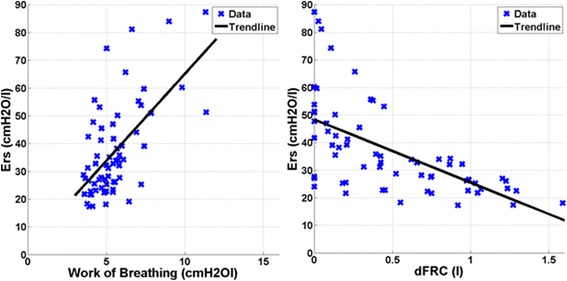
Results: Median Ers and dFRC over all patients and PEEP values were 32.2 cmH2O/l [interquartile range (IQR) 25.0-45.9] and 0.42 l [IQR 0.11-0.87]. These wide ranges reflect patient heterogeneity and variable response to PEEP. The level of PEEP associated with minimum Ers corresponds to a high change of functional residual capacity, representing the balance between recruitment and minimizing the risk of overdistension.
Conclusions: Monitoring patient-specific Ers can provide clinical insight to patient-specific condition and response to PEEP settings. The level of PEEP associated with minimum-Ers can be identified for each patient using a stepwise PEEP recruitment manoeuvre. This 'minimum elastance PEEP' may represent a patient-specific optimal setting during mechanical ventilation.
Trial registration: Australian New Zealand Clinical Trials Registry: ACTRN12611001179921.
Keywords: ARDS; Dynamic functional residual capacity; Mechanical ventilation; PEEP; Respiratory elastance.
Figures
Similar articles
-
Model-based PEEP optimisation in mechanical ventilation.Biomed Eng Online. 2011 Dec 23;10:111. doi: 10.1186/1475-925X-10-111. Biomed Eng Online. 2011. PMID: 22196749 Free PMC article.
-
Positive end-expiratory pressure at minimal respiratory elastance represents the best compromise between mechanical stress and lung aeration in oleic acid induced lung injury.Crit Care. 2007;11(4):R86. doi: 10.1186/cc6093. Crit Care. 2007. PMID: 17688701 Free PMC article.
-
Lung Recruitment in Obese Patients with Acute Respiratory Distress Syndrome.Anesthesiology. 2019 May;130(5):791-803. doi: 10.1097/ALN.0000000000002638. Anesthesiology. 2019. PMID: 30844949
-
Lung recruitment maneuvers in acute respiratory distress syndrome and facilitating resolution.Crit Care Med. 2003 Apr;31(4 Suppl):S265-71. doi: 10.1097/01.CCM.0000057902.29449.29. Crit Care Med. 2003. PMID: 12682451 Review.
-
Lung recruitment maneuvers in acute respiratory distress syndrome.Respir Care Clin N Am. 2003 Dec;9(4):401-18, vii. doi: 10.1016/s1078-5337(03)00032-7. Respir Care Clin N Am. 2003. PMID: 14984063 Review.
Cited by
-
Optimising mechanical ventilation through model-based methods and automation.Annu Rev Control. 2019;48:369-382. doi: 10.1016/j.arcontrol.2019.05.001. Epub 2019 May 7. Annu Rev Control. 2019. PMID: 36911536 Free PMC article. Review.
-
Model-based patient matching for in-parallel pressure-controlled ventilation.Biomed Eng Online. 2022 Feb 9;21(1):11. doi: 10.1186/s12938-022-00983-y. Biomed Eng Online. 2022. PMID: 35139858 Free PMC article.
-
Assessing the Asynchrony Event Based on the Ventilation Mode for Mechanically Ventilated Patients in ICU.Bioengineering (Basel). 2021 Dec 18;8(12):222. doi: 10.3390/bioengineering8120222. Bioengineering (Basel). 2021. PMID: 34940375 Free PMC article.
-
Model-based PEEP titration versus standard practice in mechanical ventilation: a randomised controlled trial.Trials. 2020 Feb 1;21(1):130. doi: 10.1186/s13063-019-4035-7. Trials. 2020. PMID: 32007099 Free PMC article.
-
Automated evaluation of typical patient-ventilator asynchronies based on lung hysteretic responses.Biomed Eng Online. 2023 Oct 24;22(1):102. doi: 10.1186/s12938-023-01165-0. Biomed Eng Online. 2023. PMID: 37875890 Free PMC article.
References
-
- Slutsky AS. Lung injury caused by mechanical ventilation*. Chest. 1999;116(suppl 1):9S–15S. - PubMed
-
- Esteban A, Anzueto A, Frutos F, Alia I, Brochard L, Stewart T, et al. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA. 2002;287(3):345–55. - PubMed
-
- Gajic O, Dara SI, Mendez JL, Adesanya AO, Festic E, Caples SM, et al. Ventilator-associated lung injury in patients without acute lung injury at the onset of mechanical ventilation *. Crit Care Med. 2004;32(9):1817–24. - PubMed
-
- Gullo A, Berlot G, Garcia CSNB, Rocco PRM, Zin WA. Understanding the mechanism of ventilator-induced lung injury. Perioperative and critical care medicine. Milan: Springer; 2006. pp. 43–59.
-
- Girard TD, Bernard GR. Mechanical ventilation in ARDS. Chest. 2007;131(3):921–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
