

Proliferative Vitreoretinopathy in Treated Retinoblastoma
- PMID: 28435935
- PMCID: PMC5396968
- DOI: 10.1016/j.oret.2016.09.009
Proliferative Vitreoretinopathy in Treated Retinoblastoma
Abstract
Objective: To evaluate the clinical and histopathologic characteristics of patients who develop proliferative vitreoretinopathy after retinoblastoma treatment.
Design: Retrospective review of three cases of proliferative vitreoretinopathy (PVR) that developed after successful treatment of retinoblastoma from 2003 to 2015.
Subjects: Three patients with treated retinoblastoma who developed severe PVR and required enucleation.
Methods: Review of clinical charts, fundus drawings, Ret-Cam 3 images, and histopathology specimens.
Main outcome measures: Clinical and histopathologic characterization of PVR in treated retinoblastoma.
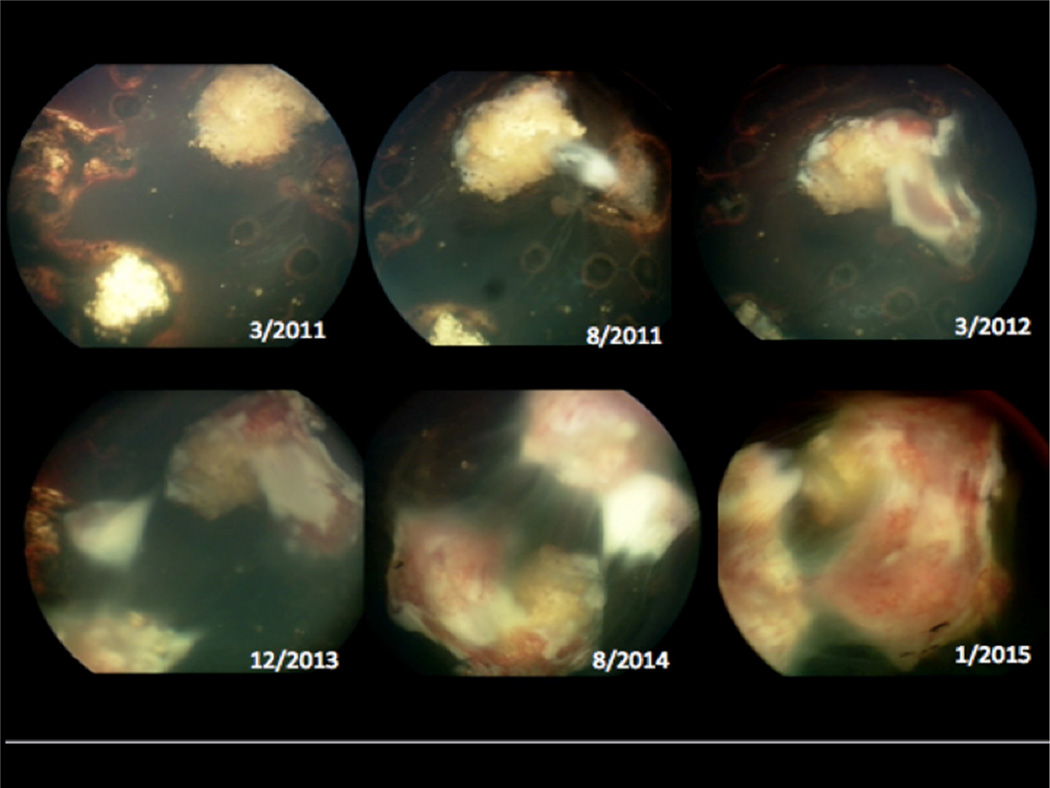
Results: Three patients developed severe PVR after sequential thermal laser combined with systemic chemotherapy for retinoblastoma. At presentation patients were 6, 7, and 9 months of age, and all had bilateral retinoblastoma. Time to development of proliferative tissue was 9, 12, and 20 months after initial treatment. Proliferation was characterized by progressive growth of white vascularized tissue with associated traction on the retina and sometimes hemorrhage. All patients underwent enucleation. Histopathologic evaluation revealed treated retinoblastoma tumor with a Type 3 regression pattern, pre- and subretinal fibrovascular tissue consistent with PVR, and reactive changes in the retinal pigment epithelium. None of the patients developed recurrence of retinoblastoma or systemic metastasis.
Conclusion: PVR uncommonly develops after successful treatment of retinoblastoma and may result in traction or rhegmatogenous retinal detachment along with vitreous hemorrhage. Early stages of proliferation may be difficult to distinguish from recurrent tumor. Enucleation may be required due to poor vision and inability to adequately monitor for tumor recurrence.
Figures






References
-
- Shields CL, De Potter P, Himelstein BP, et al. Chemoreduction in the initial management of intraocular retinoblastoma. Arch Ophthalmol. 1996;114(11):1330–1338. - PubMed
-
- Shields CL, Mashayekhi A, Au AK, et al. The international classification of retinoblastoma predicts chemoreduction success. Ophthalmol. 2006;113:2276. - PubMed
-
- Warden SM, Mukai S. Pars plana vitrectomy in eyes treated for retinoblastoma. Retina. 2006;26(7):S53–S56. - PubMed
-
- Tawansy KA, Samuel MA, Shammas M, et al. Vitreoretinal complications of retinoblastoma treatment. Retina. 2006;26(7):S47–S52. - PubMed
-
- Yokoi T, Hiraoka M, Suzuki Y, et al. Glial extrusion from regressed retinoblastoma after conservative treatment. Acta Ophthalmol. 2008:462–464. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials